
Table of Contents:

Introduction
Trans·gen·der - adjective
Denoting or relating to a person whose sense of personal identity and gender does not correspond with their sex assigned at birth.
In cultures worldwide, for as long as human civilization has existed, there have been people whose experience of their gender identity do not align with the Anglo-European concepts of binary sex based on genital structure. The Gala, a middle gender priest class of the Sumerian empire, existed over 4,500 years ago. Many of the Indigenous cultures of North America recognized a third gender far before European colonialism, and still do to this day. Tribal cultures all across Africa recognize numerous gender identities, which Europeans tried to wipe out. Human beings have long lived with identities, norms, and degrees of conformity to those norms which differ from the so-called “traditional” idea of gender in westernized culture today.
In spite of this, however, the modern western understanding of the transgender experience has only existed for approximately 130 years. Even the word “transgender” only dates back to 1965, when John Oliven proposed it as a more accurate alternative to David Cauldwell’s term “transsexual” (coined in 1949), which itself replaced Magnus Hirschfeld’s term “transvestite” (1910).
Being transgender can mean that a person born with a penis is actually a girl, that a person born with a vulva is actually a boy, or that a person with any genital configuration may not wholly fit either side of that spectrum and is non-binary.
A trans person can come to recognize this at any point in their life. Some children identify it at as soon as they are able to grasp the concept of gender, others don’t start to feel anything until the onset of puberty, and still others do not realize that anything is wrong at all until they are fully adults. Many people are simply never exposed to the idea that their gender could mismatch their sex assigned at birth, or what that feels like, and thus have simply accepted their fate.
Even more common is a perception wherein, even though someone may have feelings about being unhappy with the gender they were assigned at birth, they believe that this is not the same as what transgender people experience. Some may feel that a wish to be transgender and have transition available is some kind of disrespect towards “real” trans people who knew they were actually boys or girls “born in the wrong body.” These narratives of the transgender experience that have been spread by popular media can create a very false impression of just what it means to be transgender and what growing up transgender feels like.
This experience of discontinuity between the societal presumed gender and the internal sense of self is what we describe as gender dysphoria, and is common among nearly all trans individuals, regardless of their position within or outside of the gender binary. This has at times been something of a political topic within trans communities, as different groups have their own ideas of what gender dysphoria is, how it manifests itself, and what qualifies a person as being trans. So as not to get lost in that topic, this site will define gender dysphoria in broad terms of incongruence with sex assigned at birth. If you experience gender identity in a way that does not match what was assigned to you at birth, your claim to the transgender identity is valid, no matter how that incongruence manifests for you.
The purpose of this site is to document the many ways that gender dysphoria can manifest, as well as the numerous forms of gender transition, in order to provide a guide for those who are questioning, those who are starting their transgender journey, those already on their path, and those who simply wish to be better allies.


What is Gender?
Gen·der - Noun
The range of characteristics pertaining to, and differentiating between, femininity and masculinity. Depending on the context, these characteristics may include biological sex, sex-based social structures (i.e., gender roles), or gender identity (the personal sense of one's own gender).
If you trace the etymology of the word to its Latin roots, gender simply means “type”. The Norman French term gendre was in use in the 12th century to describe “the quality of being male or female.”
Many people attribute the term to psychologist John Money, who proposed using “gender” in 1955 to differentiate mental sex from physical sex. However, Money was not the first to do so. Cultural anthropologist Margaret Mead used the term in 1949 in her book Male and Female to distinguish gendered behaviors and roles from biological sex. The American Journal of Psychology (vol. 63, no. 2, 1950, pp. 312) described the book thusly:
A book, moreover, which gives beyond its premise; for it informs the reader upon ‘gender’ as well as upon ‘sex,’ upon masculine and feminine roles as well as upon male and female and their reproductive functions.
Margaret Mead moves from the specific delineation to the more general comparison of male and female in several communities, finally coming to an analysis of sex-patterns in our own midst and for our own time.
 Cog
Cog 
 Darkly Dai (Now with added werewolf)
Darkly Dai (Now with added werewolf) 
Human Sex (the adjective, not the verb) is broken down into three categories:
- Genotype: The genetically-defined chromosomal kareotype of an organism (XX, XY, and all variants thereof)
- Phenotype: The observable primary and secondary sexual characteristics (genitals, fat and muscle distribution, bone structure, etc.)
- Gender: The unobservable sexual characteristics, the internal mental model of a person’s own sex, and the way that they express it.
Any of these three aspects can fall into a position on a range of values. Your elementary school health class probably taught you that genotype is binary, either female (XX) or male (XY), when the reality is that there are a dozen other permutations that can occur within human beings.
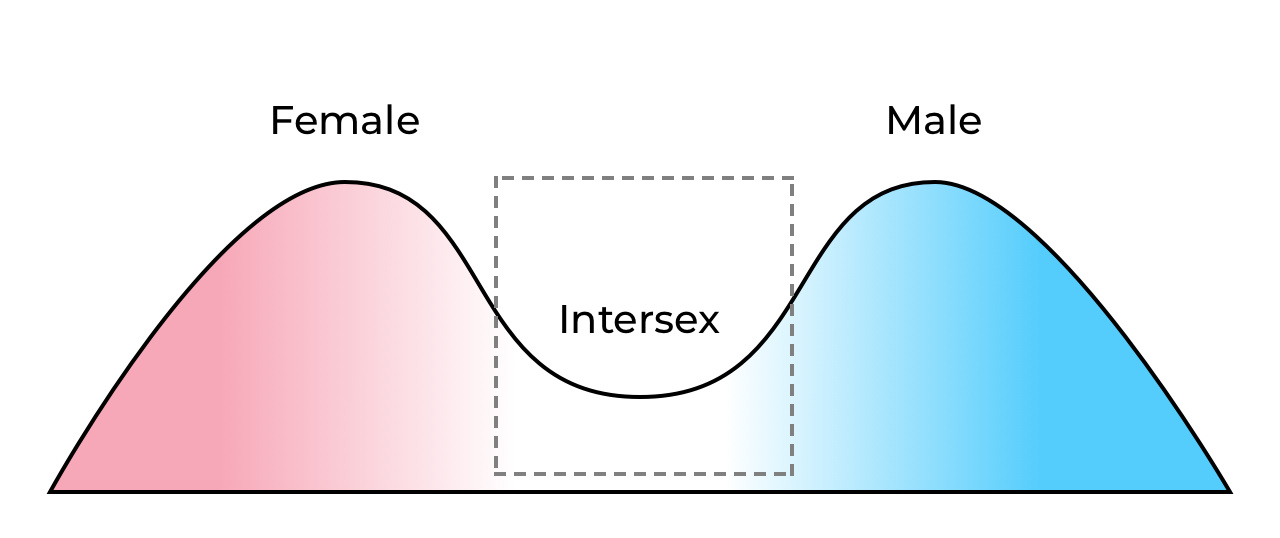
Likewise, many people believe that phenotype is also binary, but biology has recognized for hundreds of years that, when you plot out all sexual characteristics across a population, you actually end up with a bimodal distribution where the majority of the population falls within a percentile of two groups. This means that some people will, simply by nature of how life works, fall outside of the typical two piles. Many people fall in the middle, with characteristics of both sexes.
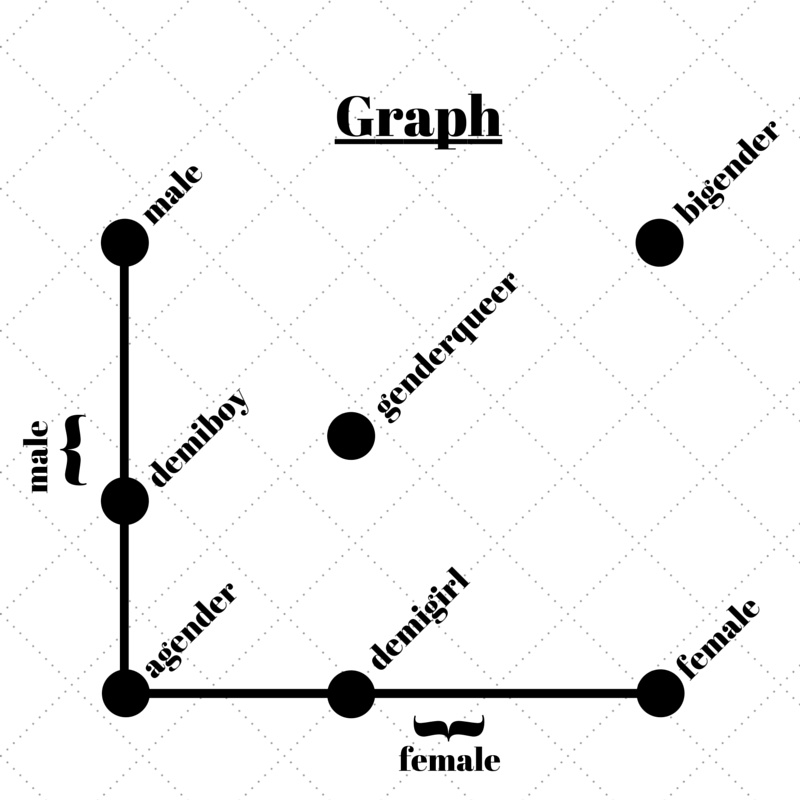
Gender, however, is a lot more… esoteric. There are a lot of different ways in which people have attempted to illustrate a gender spectrum, but none have quite thoroughly captured it because the breadth of what gender encapsulates is itself a very abstract concept.
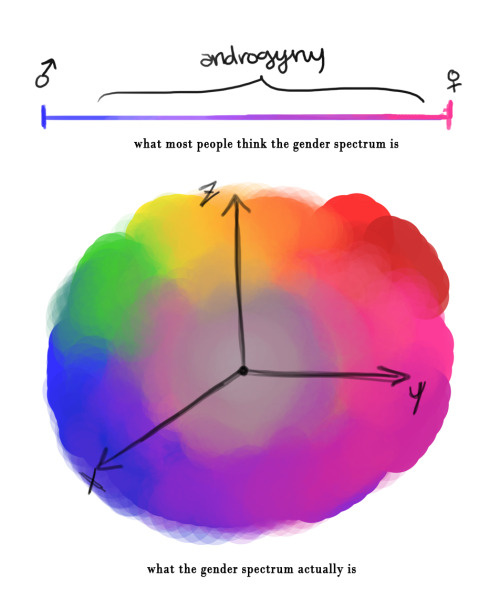
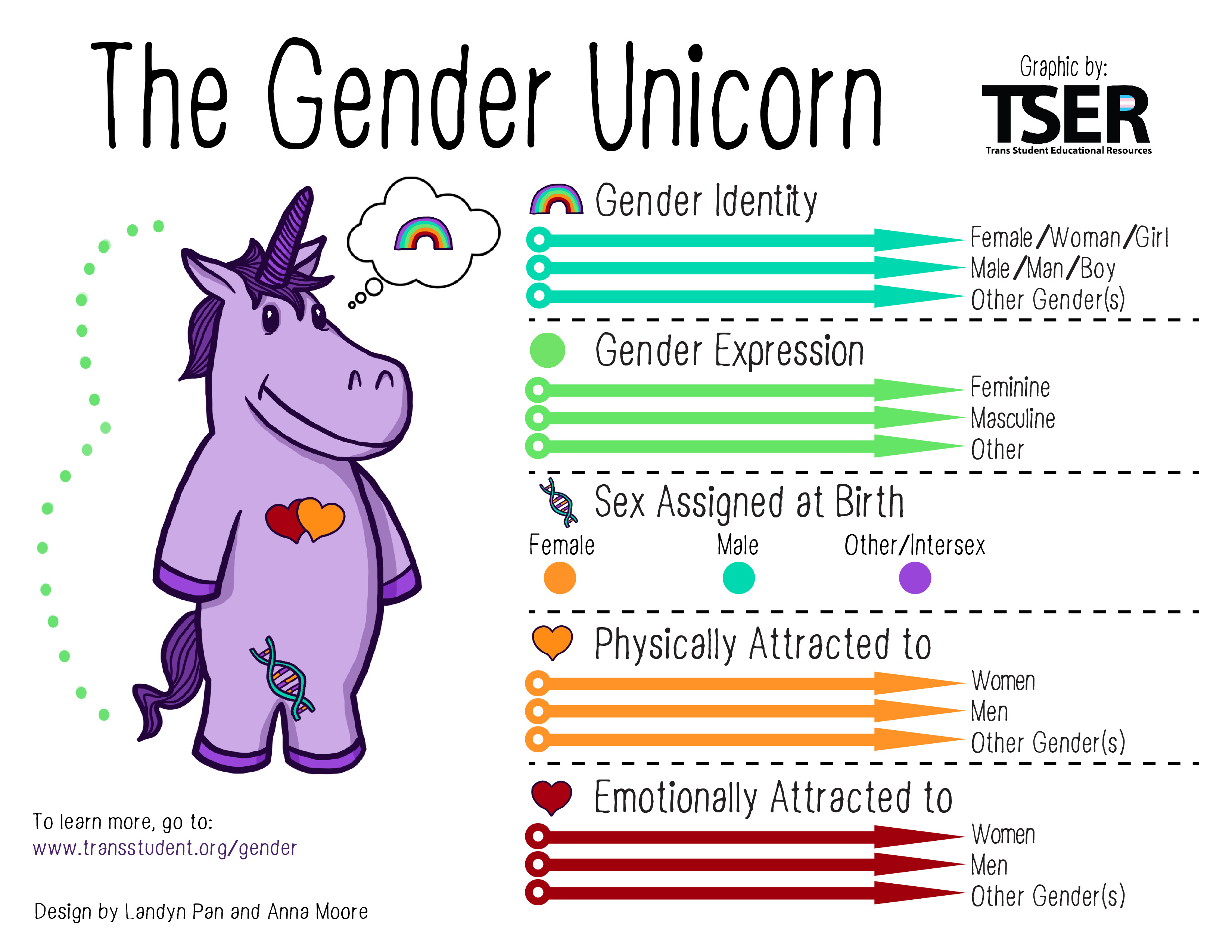
Sources: [Tumblr] [TransStudent.org]
The short of it is: some people are very male, some people are very female. Some people feel no gender at all, some people feel both. Some feel their gender weakly, others feel it intensely. Some people oscillate all over the spectrum in unpredictable ways, changing like the wind. Some might question the premise of a spectrum at all! Only an individual can identify their own gender; no one else can dictate it for them.
Gender is part social construct, part learned behaviors, and part biological processes which form very early in a person’s life.
Present evidence seems to suggest that a person’s gender is established during gestation while the cerebral cortex of the brain is forming (more about that in the Causes of Gender Dysphoria section). This mental model then informs, at a subconscious level, what aspects of the gender spectrum a person will lean towards. It affects behavior, perceptions of the world, the way we experience attraction (separate from sexual orientation and hormonal influences) and how we bond with other people. These may not all line up the same way.
Gender also affects the expectations that the brain has for the environment it resides in (your body), and when that environment does not meet those expectations, the brain sends up warning alarms in the form of depression, depersonalization, derealization, and dissociation. These are the brain’s subconscious ways of informing us that something is very wrong.
Hab·i·tus - Noun
Socially ingrained habits, skills, and dispositions. The way a person perceives and reacts to the world.
On the social side, gender involves our habitus: our presentation, our mannerisms and behaviors, how we communicate, how we react, what our expectations are from life, and the roles that we fulfill as we walk through life. The author Susan Stryker described habitus it in her book Transgender History:
A lot of habitus involves manipulating our secondary sex characteristics to communicate to others our own sense of who we feel we are—whether we sway our hips, talk with our hands, bulk up at the gym, grow out our hair, wearclothing with a neckline that emphasizes our cleavage, shave our armpits, allow stubble to be visible on our faces, or speak with a rising or falling inflection at the end of sentences. Often these ways of moving and styling have become so internalized that we think of them as natural even though—given that they are all things we’ve learned through observation and practice—they can be better understood as culturally acquired “second nature.”
Indeed, these are all cultural factors: things which have developed within the population over time. Regardless of being essentially “made up”, they are still strongly gendered and a person tends to connect to the gendered habitus of their internal self without even realizing they are doing it. When we are denied access to those social aspects, this results in discomfort with one’s social position in life.
John Money’s experiments attempted to confirm his belief that gender is entirely a social construct, and that any child can be raised to believe themselves to be whatever they were taught to be. His experiment was a massive failure (see the Biochemical Dysphoria section). Gender does not change; every human is the same gender at 40 that they were at 4. What changes is our own personal understanding of our gender as we mature as individuals.
These negative symptoms (depression, derealization, social discomfort) are the symptoms of Gender Dysphoria.
What Gender is not is sexual orientation. We describe orientation using terms relative to one’s gender (homosexual/heterosexual/bisexual, etc), but gender itself does not affect sexuality and sexuality has no role in gender.
What does it mean to be Non-binary?
Non-binary identities are outside of an exclusive affinity to either male or female. Sometimes this means a total affinity to both (bigender) or balanced affinity to both (androgyne). It can also mean an affinity that changes from day to day (genderfluid), a partial affinity (demigender), or even an affinity to the entire gender spectrum at once (pangender).
It can also mean a lack of affinity to any gender identity at all (agender) or a strong affinity to a gender identity that isn’t relative to either male or female (including but not limited to aporagender).
Some non-binary people have an affinity to some aspects of a gender but not others. For example, a demigirl could be someone assigned female at birth who only feels a partial connection to womanhood and femininity, or may be a male-assigned individual who is taking hormone therapy to relieve physical dysphoria, and has a female phenotype, but does not experience a strong connection to the social aspects of womanhood.
In generalist terms, this book will be describing gender in a sense of binary identities (male/female) vs non-binary identities, but this is purely for the sake of writing simplicity. Similarly, the list of non-binary identities mentioned is not exhaustive. Please know that the depth of gender experience and expression is far, far more complicated than this simple breakdown.
A Brief History of Gender Dysphoria
In 1948, noted sexologist Dr. Alfred Kinsey (yes, that Kinsey) was contacted by a woman whose male child adamantly insisted that they were in fact a girl, and that something had gone very wrong. The mother, rather than trying to suppress her daughter, wished to help her become who she knew herself to be. Kinsey reached out to a German endocrinologist named Dr. Harry Benjamin to see if he could help the child. Dr. Benjamin then developed a protocol of estrogen therapy for the teen, and worked with the family to find surgical help.
Benjamin then went on to refine his protocol and treated thousands of patients with similar feelings over the course of his career. He refused to take payment for his work, instead taking satisfaction from the relief he granted these patients, and using their treatment to further his understanding of the condition. He coined a term for this feeling of incongruence in 1973: gender dysphoria. Unfortunately, this term would not be used in the United States until 2013, with the American Psychiatric Association opting for the term “gender identity disorder” instead.
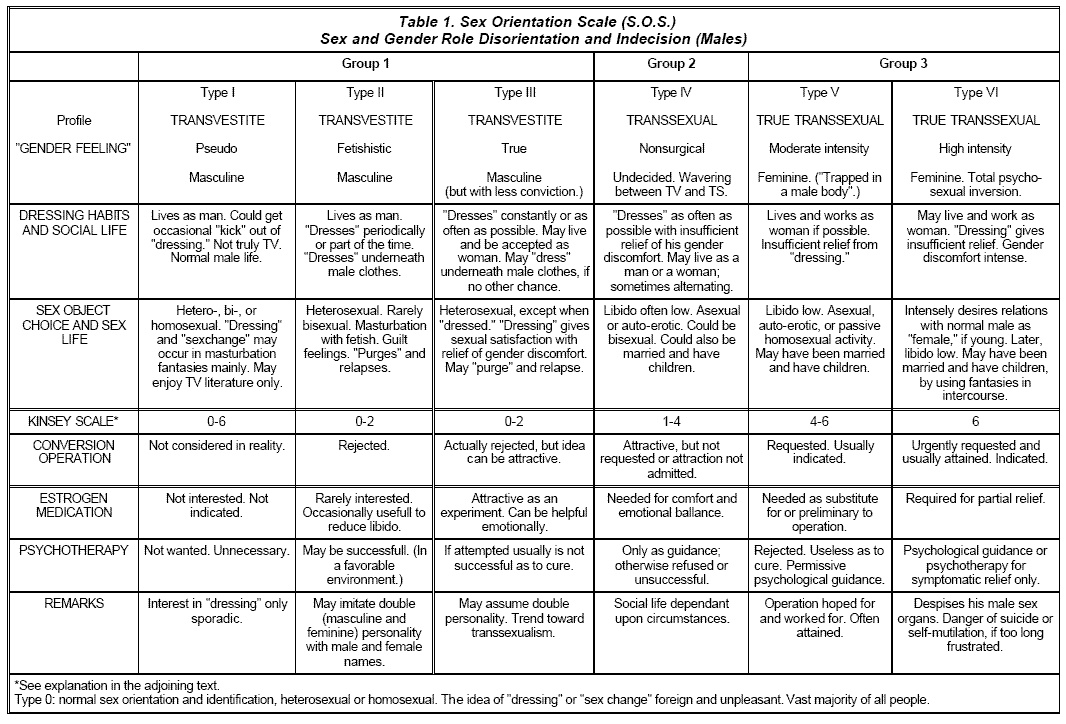 Harry Benjamin Diagnostic Scale
Harry Benjamin Diagnostic Scale If you are a trans person reading this, you may have heard the name Harry Benjamin before, but probably not in a favorable context. In 1979 his name was used (with permission) in the forming of the Harry Benjamin International Gender Dysphoria Association (HBIGDA), which released a Standards of Care (SoC) for transgender people. This SoC came to be known as the Harry Benjamin Rules, and were infamously limiting in regards to how gender dysphoria could be diagnosed. Patients were placed within a six tier scale based upon their level of misery and sexual dysfunction. If you did not land at Tier 5 or higher, classified as a “True Transsexual”, you were usually rejected for treatment.
The problem was that Tiers 5 and 6 required that you had to be exclusively attracted to your own birth sex. Transition had to be making you straight, not gay, and bisexuals were not allowed. You also had to be experiencing severe distress with your body and genitals and already be living as your true gender without treatment. Many trans people got around these limitations through community coaching and performative presentations, but for many people (myself included) it was believed that, if you did not fit all the criteria, you were not trans enough to transition.
In 2011, the HBIGDA reorganized itself to respond to mounting pressures in trans understanding and acceptance, taking on the new name World Professional Association for Transgender Health (WPATH). Under guidance by actual transgender people (a first for the organization), WPATH then proceeded to release an entirely new Standards of Care (SoC, version 7, the first in ten years) which abandoned the Benjamin Scale, focusing on specific individual symptoms and disconnecting gender from sexuality entirely. Two years later, in 2013, the American Psychiatric Association changed their diagnostic criteria to match the WPATH SoC in their Diagnostic and Statistical Manual of Mental Disorders (DSM) version 5, replacing Gender Identity Disorder with Gender Dysphoria. With this change, medical transition became available to all trans people in the United States.
This is why trans presence across the world has suddenly exploded in the last decade. With easier access comes larger numbers, with larger numbers comes more visibility, with more visibility comes more awareness, and with more awareness comes more people accessing treatment. A study conducted in 2014 showed 0.6% of adults and 0.7% of youth in the United States identified as transgender, a study conducted in 2016 showed 1.8% of high school age students identified as transgender, and a survey conducted by GLAAD in 2017 showed a whopping 12% of respondents 18 to 34 did not identify as cisgender.
Transgender people are coming out of the woodwork; we are everywhere.
So What Is Gender Dysphoria?
Dys·pho·ri·a - Noun
A state of unease or generalized dissatisfaction with life. The opposite of euphoria.

There is a common misconception among both cisgender and transgender people that gender dysphoria refers exclusively to a physical discomfort with ones own body. However, this belief that body discomfort is central to gender dysphoria is in fact a misconception, and is not even a majority component of a gender dysphoria diagnosis. Gender dysphoria crosses a large number of all aspects of life, including how you interact with others, how others interact with you, how you dress, how you behave, how you fit into society, how you perceive the world around you, and, yes, how you relate to your own body. Consequently, proponents of the WPATH SoC 7 and the DSM-5 have taken to a habit of saying that you do not have to have dysphoria to be transgender. This statement is often repeated like a mantra, as it informs people who do not feel significant body discomfort that they may also be transgender.
In principle, gender dysphoria is a feeling of wrongness intrinsic to the self. There is no logical backing to this wrongness; there is nothing which explains it, and you can not describe why you feel this way; it is just there. Things in your existence are incorrect, and even knowing which things are incorrect can be hard to properly identify.
The way I used to describe it is like wearing an adult’s glove when you are a child. You can put your hand into the glove, and your fingers feed into the digits of the glove, but your dexterity with the glove is severely hindered. You might be able to pick something up, but you can not manipulate it like an adult could. Things just aren’t quite right.
Evey Winters described it this way in her Dysphoria post.
Have you ever been sitting somewhere in a public or a formal place and all of a sudden the bottom of your foot itches? It’s not like you can remove your shoes right there and scratch it, so you endure the feeling of dying inside while this itch grows and grows until you are ready to murder the next person that speaks to you.
Or when I was younger I used to watch cable TV in the mornings before school. Because it was cable TV in rural WV in the early 90’s, every so often I’d turn on my favorite channel to watch my shows while I ate my maple oatmeal and I’d be seeing Power Rangers — but the audio would be from another station (usually the weather channel). The video was fine. The audio was fine. But the mismatch between them? That’s the kind of frustration that sits with you all day as a child.
It’s the feeling you get when you ask for a crisp refreshing Diet Coke and the server says, “Is Pepsi ok?”
It is knowing that something is wrong and not being able to do a damn thing about it.
Gender dysphoria is, at its core, simply emotional reactions to the brain knowing that something does not fit. This incongruence is so deep inside the brain’s subsystems that there is no obvious message of what the problem is. The only way we have to identify it is via the emotions that it triggers. Our consciousness receives either positive (euphoria) or negative (dysphoria) feedback according to how well our current environment aligns with our internal sense of self. Part of transition is learning to recognize those signals.
Cisgender people receive them as well, but since the signals usually align with their environment, they take them for granted. There have been a few notable occasions, however, when a cisgender person has been put into a situation where they experience gender dysphoria. Attempts to raise cisgender children as the opposite sex (Content warning: suicide) have always met with failure when the child inevitably declares themselves differently.
These impulses of euphoria and dysphoria, arousal and aversion — they all manifest in many different ways: some obvious, some much more subtle. Dysphoria changes over time as well, taking on new shapes as one moves from pre-awareness into understanding and through transition. The goal of this book is to break down these manifestations into their distinct categories and describe them so that others may learn to recognize them.
However, first I must stress something very important, so important that I am putting it into big bold letters:
EVERY SINGLE TRANS PERSON EXPERIENCES A DIFFERENT SET OF DYSPHORIA SOURCES AND INTENSITIES
There is no one single trans experience; there is no standard set of feelings and discomforts; there is no one true trans narrative. Every trans person experiences dysphoria in their own way to their own degree, and what bothers one person may not bother another.
Okay, with that disclaimer out of the way, let’s get to the meat and potatoes.
Gender Euphoria
Eu·pho·ri·a - Noun
A feeling or state of intense excitement and happiness. Elation, joy, glee.
Before I can talk about discomfort, I have to talk about relief. Gender euphoria is itself a sign of gender dysphoria. You might be asking yourself, “how can happiness be sadness?” The answer to that is simple.
Imagine a person who was born in a cave, who spent their entire life living underground, with their only source of illumination being candles and oil lamps. Imagine they’ve never been above ground; they don’t even know the surface exists. Then, one day, a cave-in happens in a side tunnel, and reveals an opening to the surface. Sunlight pours into the opening, and at first it is blinding and the person runs away in fear. Later, they return to the opening, and, as the person’s eyes adjust, they look out through the hole and see a bright and brilliant world full of colors they didn’t even know existed.
That world is scary, huge, and full of unknowns, so they crawl back into the cave for safety, but that hole is still there, and they see the light every time they pass it. Gradually, they peek out more and more frequently, and further and further from the opening. They start to want that light; they find reasons to visit it more often.
Eventually they realize that they don’t want to go back into the hole any more. They have to go back, because that is where their family and friends are, but this place is so much better, and they want to stay here. Going back into the hole feels wrong; it starts to hurt to be in the dark so much.
This is what gender euphoria is like: brief flashes of a light that may be too bright to handle at first, too confusing to understand, but as time goes on you become more accustomed to them and you realize that this is where you belong, and the darkness becomes the dysphoria.
Many trans people have no idea how much pain they are in until they find small bits of relief. Cosplay, stage acting, drag, role playing games, video games; small little forays into a different gender than they have lived as. They find that it feels just a little bit more comfortable. They’ll make up excuses for why (“If I’m gonna be looking at this character’s ass, it might as well be a girl’s ass.”), they’ll try to convince themselves it’s all just for fun, or an artistic expression. They might tell themselves that the bits of joy they feel at hearing a different pronoun are just novelty. But soon they find themselves looking for reasons to get that more often. More and more frequently they’re role playing characters of a different sex, building more costumes, buying more clothes, performing more often. You find yourself wanting to do that all the time, because it just feels better than your real life, and being “you” starts to hurt. Eventually, the old you becomes the costume.
This is the most fundamental reason why we as a community say “you do not need dysphoria to be trans”, because black ink on a black canvas isn’t visible without close examination and a lot of light.
Anything that can be a source of dysphoria has an equal and opposite euphoria.
 Erin, Sundresses Mom
Erin, Sundresses Mom Examples:
- Being gendered correctly
- Being addressed by your chosen name
- Wearing correctly-gendered clothing
- Seeing and feeling changes in your body
- Seeing yourself in the mirror (removal of depersonalization)
- Socializing in a way that conforms with gendered expectations
- Getting a haircut in a masculine / feminine / androgynous manner
- Shaving your legs
- NOT shaving your legs
- Being included in something you wouldn’t otherwise because of your assigned gender (e.g. bridal shower or bachelor party)
- Feeling sexy / having sex in a way that aligns with your gender and sexuality.
Even just being out in the world as yourself and being seen as yourself can be massively euphoric.
What euphoria is NOT is a sexual high, turn-on, or fetish. Sometimes euphoria can trigger a sexual response, and there are many factors at play that cause that (feeling good about your body is a turn-on, for example), but it is not a source of sexual excitement. Trans people are not “getting off” on presenting or acting like their true selves.
That said, many people who have not yet realized they are trans may resort to fetishes and kinks to express their gender and/or relieve their dysphoria. They may maintain some of these kinks through transition. There is no shame in this; how they find sexual fulfillment is their own business. However, these things are alongside their gender. A trans person’s sense of gender persists indefinitely; it does not go away when they go back to their daily lives.
Physical Gender Dysphoria
Everyone has heard of the “born in the wrong body” narrative. Physical dysphoria is discomfort over the shape of one’s body due to the sexual characteristics it presents. So what body features are we talking about here?
Primary Sex Characteristics
The core reproductive features which develop during pregnancy
- Gonads
- Testicles
- Ovaries
- External Genitalia
- Penis
- Clitoris
- Scrotum
- Labia
- Vulva
- Internal Reproductive Organs
- Prostate / Skene’s Gland
- Uterus
Secondary Sexual Characteristics
All sexually dimorphic features which develop during and after puberty as a result of hormone exposure. In general, these features are all nearly identical for both male and female prepubescent children.
- Fat Distribution
- Waist, Hips, Butt Shape
- Thighs, Arms, Back
- Cheeks and Jaw Line
- Muscle Mass
- Neck, Shoulders and Upper Body
- Arms and Legs
- Abdominal
- Skeletal Build
- Range of Height
- Size of Feet and Hands
- Width of Shoulders
- Rib Cage Breadth
- Thickness and Density of Limbs
- Forehead, Brow, Cheek and Jaw bones
- Pelvic Width
- Skin Texture and Tone
- Voice Pitch and Resonance
- Breast Development
- Facial Hair
- Body Hair (excluding genitals and arm pits)
For Your Information
The genitals of a transgender person on hormone therapy do not behave remotely like their cisgender counterparts.
-
The estrogenic penis softens, erections become less pronounced, and the skin thins and begins to perspire like a vaginal wall. The scrotum softens and changes color, with the perineal raphe becoming more distinct. Due to the cessation of random erections, the erectile tissue will atrophy if not regularly put to use, causing the entire penis to shrink over time. Vibration becomes more effective for arousal.
-
The androgenic vagina becomes drier & prone to tearing (lubrication can be an issue). The skin of the clitoris thickens, and the clitoral glans grows in length and girth due to the onset of random erections. Labia also become thicker, and often hairier. The onset of HRT often results in extreme sensitivity of the clitoris. Friction becomes more effective for arousal.
Primary characteristics can only be altered through surgical intervention. Some secondary sexual characteristics are also one-way trips and require medical intervention to undo, namely the growth of breast tissue and the deepening of the vocal chords. Estrogen does not make the voice more feminine, and testosterone does not make breasts shrink (aside from the loss of fat). Changes to skeletal structure (such as enlarging from testosterone and the widening of hips from estrogen) can only occur prior to the age of 25, while the body is still growing.
Some secondary traits can be surgically enhanced (breast augmentation, body contouring, facial masculinization / feminization), and some cannot be changed at all.
Physical dysphoria manifests in several different ways. Sometimes this is felt in a sort of phantom limb phenomenon, where the person can feel sensations from a penis or vagina that is not there, an ache in a uterus that does not exist, or a sense of absence on the chest from breasts that have not grown in.
It can be felt as a sort of reverse phantom effect, where the person is persistently aware of something that should not be there. The brain is receiving sensory input that it does not expect, such as the weight of breasts, or the presence of testicles or a uterus, and this input takes priority because it isn’t expected.
It may be felt as horror or revulsion when looking at or touching the external genitals, triggering emotional outbursts or a strong desire to remove the offending organ. AFAB (assigned female at birth) trans people may experience feelings of wrongness during menstruation, or a sense of alien disconnect from their hormone cycle.
 Not Even a Chef
Not Even a Chef It can manifest as a compulsion to be rid of certain body traits, such as obsessively shaving body or facial hair. This can also manifest in the opposite compulsion, leading to meticulous grooming of those traits in order to try to control them, like maintaining a perfect beard, persistently keeping one’s nails manicured and polished, or spending hours in the gym attempting to hone one’s shape.
Undesired physical features may prompt a person to experience envy of people who have been forced to remove those features due to illnesses, such as testicular or breast cancer. AMABs with severe genital dysphoria tend to have a wish for some kind of freak accident that would cause the loss of their phallus.
Sometimes it may just simply be a feeling of being incorrect, which you may not even attribute to gender or sex. For most of my life, I believed that the reason I hate my body was because I was fat. It wasn’t until I started transition that I realized I don’t hate my fat at all; I hated having male fat. The feminine curves that HRT gave me make me feel so much more in tune with my body.
 To My Side My Noble Pandherjar
To My Side My Noble Pandherjar The dysphoria one feels about their body can and will change over time, for better and worse. For example, many trans women enter into transition feeling no disconnect with their genitals, but later find that as larger sources of dysphoria melt away, that they become less comfortable with their original configuration. Alternatively, some may assume that they will absolutely need facial feminization surgery, but then, two years into transition, realize they’re actually okay with how they look.
It’s okay for you to realize you need more or less than when you started.
It’s okay if you don’t hate anything about your body and just wish you looked more feminine or masculine.
It’s okay if you only hate some aspects of your body and don’t wish to change all of its sexual characteristics.
It’s okay if you don’t need medical transition at all. Body feelings are not the be-all-end-all of transition.
Total body physical dysphoria is not a requirement to be transgender. AFABs do not have to hate their chest, AMABs do not have to hate their penis. Every trans person’s experience is different. All are valid.
Internalized Body Image Issues
The world is full of subconscious messages about how men and women’s bodies should be shaped. We are bombarded with advertising and media creating a normalized view of what is and is not beautiful. Don’t be too fat, don’t be too skinny, don’t be too tall, don’t be too short, don’t have too broad of a chin, don’t have too large of a nose, wear makeup but don’t wear too much makeup, don’t leave the house without a bra, but don’t let the bra show. On and on and on, the constant barrage of expectations of gendered appearance.
Everyone absorbs these messages, and trans people internalize the factors which matter to the gender they align with. Those who align with femininity grow up mapping feminine standards onto themselves, those who align with masculinity map masculine standards on to themselves, and non-binary people may internalize shame around androgyny or the gender they are assumed to be after transition. This is on top of the shame trans people in general are loaded with for not living up to their assigned gender’s standards.
What is the end result of this? Kathryn said it best:
 Kathryn Gibes
Kathryn Gibes  @TransSalamander
@TransSalamander If you're under the assumption that you're a cis guy but have always dreamed of being a girl, and the only reason you haven't transitioned is because you're afraid you'll be an "ugly" girl:
That's dysphoria. You're literally a trans girl already, hon.
Kathryn Gibes @TransSalamander Don't feel too bad about never realizing it. I just had this eureka moment myself.
But that's literally dysphoria. You feel discomfort being reminded of the disconnect between who you want to be (who you ARE) and what you look like.
Biochemical Dysphoria
The primary sexual features of the body begin development during the eighth week of human gestation. Typically, by week 11, it is possible to determine the genitals of a fetus via ultrasound. The brain, however, forms between weeks 14 and 24. Current prevailing understanding of neurological development suggests that it is during these 10 weeks when the brain will either masculinize or feminize based upon the presence of testosterone in the fetus bloodstream (initiated by the SRY gene on the Y chromosome, or introduced from other sources). This process locks the brain into a pattern of either desiring estrogens or androgens.
If your brain is wired for one kind of gonadal hormones (such as testosterone) and your body produces the other hormone (such as estradiol), this can result in a biochemical malfunction within your brain chemistry. This produces a sort of brain fog: a reduction in mental capacity and a general state of anxiety and unease. This is the source of the first two symptoms that often alleviate with medical hormonal therapy: depersonalization and derealization (DPDR).

Depersonalization is a disconnect from your own body: an inability to believe that the person you see in the mirror is actually yourself. You feel like you are watching someone else in your body. You may find yourself not caring about what happens to your body, feeling a lack of concern with weight changes or improving your fitness because you have no ownership of this fleshy vehicle that transports you around your life.
Zinnia Jones gives these descriptions for Depersonalization:
- A sense of detachment or estrangement from your own thoughts, feelings, or body: “I know I have feelings but I don’t feel them”
- Feeling split into two parts, with one going through the motions of participating in the world and one observing quietly: “There is this body that walks around and somebody else just watches”
- Feeling as if you have an “unreal” or absent self: “I have no self”
- Experiencing the world as distant, dreamlike, foggy, lifeless, colorless, artificial, like a picture with no depth, or less than real
- Being absorbed in yourself and experiencing a compulsive self-scrutiny or extreme rumination
- Having an ongoing and coherent dialog with yourself
- Feeling like a veil or glass wall separates you from the world
- Emotional or physical numbness, such as a feeling of having a head filled with cotton
- Lacking a sense of agency – feeling flat, robotic, dead, or like a “zombie”
- Inability to imagine things
- Being able to think clearly, but feeling as if some essential quality is lacking from your thoughts or experience of the world
- A sense of disconnectedness from life, impeding you from creative and open involvement with the world
You may put little care into your physical appearance, reaching for only the basic utilitarian needs in clothing and personal hygiene. Alternatively, you may hyperfocus on your appearance, attempting to try to spark some kind of joy, any kind of feeling of pride in your own body, only to be met with more hollowness.
You may be unconcerned with the state of your body, perhaps not even fearing death, because you have so little attachment to your life.
 Nightling Bug
Nightling Bug  @NightlingBug
@NightlingBug You have an underlying sense that you are "not like" most people. Your friends might get you, but you draw an instinctive and unconscious line between you and "normal" people. When you interact with a "normal" person, you're not sure what to say or how to act.
Nightling Bug @NightlingBug You find it hard to prioritize your own feelings. You're aware of emotions you *should* be feeling, but they're distant and fake-seeming. When someone else is upset, it's much more real and urgent. You believe this is just your stoic, protective nature.
Nightling Bug @NightlingBug You often feel directionless in life. When asked about career goals in High School, you didn't really care about your answer. Even careers centered in your interests seemed kind of intolerable. You struggle to imagine a future for yourself where you are happy or fulfilled.
Nightling Bug @NightlingBug You only take steps to better your life when external forces *make* you. You'd rather withdraw and self-minimize and focus on escapist hobbies. You're just not motivated to attain nice things for yourself. (You tell yourself that this is a zen acceptance, a freedom from desires.)
Derealization is a detachment from the world around you: a mental sense that everything you perceive is false.
- Your surroundings seem alien or unfamiliar, even if you’ve always been there, like someone has swapped out your house for a stage replica.
- Moving through the world feels like you’re walking on a treadmill, with the buildings moving around you instead of you through them.
- Feeling emotionally disconnected from people you care about, as if you were separated by a glass wall, or like they are just actors pretending to be the people they claim to be.
- Surroundings that appear distorted, blurry, colorless, two-dimensional or artificial, or a heightened awareness and clarity of your surroundings. Leaves on trees feel like they have extra sharp edges, for example.
- Distortions in perception of time, such as recent events feeling like distant past.
- Distortions of distance and the size and shape of objects
- Feeling like a passive observer in the events of your life
If you found yourself strongly relating to The Matrix or The Truman Show, you might be experiencing derealization. This can also manifest as a feeling of otherworldliness, like you don’t belong in this society. You’re just walking around waiting for your super powers to appear, or for an owl to fly up with your letter to Hogwarts. As a teen I was obsessed with an episode of The Outer Limits where a boy discovers a spaceship under his house and learns that he and his parents aren’t actually human.
DPDR sometimes comes with an emotional stunting. You are able to laugh and find humor, but rarely ever genuine joy. Moments of sadness or grief cause you to just go numb, dissociated by the event that caused it. This can also go in the opposite direction, where the person is under so much anxiety that their emotional response is extremely disproportionate to the catalyst, resulting in severe crying or violent outbursts from seemingly small events.
It’s important to note that DPDR is not exclusive to gender dysphoria. This condition is comorbid with several other mental health issues, including chronic depression, obsessive compulsive disorder, and borderline personality disorder. DPDR should not be taken as a sign of gender dysphoria purely on its own; it’s just a big alarm signal that something is very wrong. It’s also usually pretty easy to spot externally, once you know how to watch for it. People with DPDR tend to have a mile long stare as they move about in the world; eyes so gloomy and dead that they look like a shell. One of the most common comments on transition timelines is how the eyes gain so much spark.
The Ebb and Flow
The intensity of physical and biochemical dysphoria is highly influenced by other factors in the body. Because it is a function of endocrine balance, it is also manipulated by those balances. This means that it can rise and fall from day to day. For example:
- If your blood sugar is out of whack, or you have a thyroid condition, it could cause your dysphoria to spike.
- If you are having dopamine withdrawal because of ceasing stimulants, that can make it worse.
- If you start on an SSRI antidepressant and start running with more serotonin, that can make it less intense.
- Transfeminine AMABs (people assigned male at birth) with testicles experience surges in testosterone in relation to attraction and desire, which can make them more dysphoric.
- Transmasculine AFABs (people assigned female at birth) with unsuppressed ovaries experience rises and falls in estrogen and progesterone over the course of their menstrual cycle, making their dysphoria intensify and lessen based on what day of the cycle they are on.
There are dozens of systems in the body that all work in tandem, and they all fluctuate from day to day, manipulating general mental state. This general dysphoria can amplify the affect of all other dysphoria. One day you can shrug off misgendering like it’s nothing, and then the next it hurts like a stab in the heart every time. One day you see yourself in the mirror, the next you’re staring at the old you.
Some people experience this in a genderfluid way, with some days leaning male, some days leaning female, and other days not feeling any gender, or both. Others just feel it like a seasonal river; sometimes it swells because of rains up stream, sometimes it slows to a trickle because of drought.
All of this is valid, and just because you feel very dysphoric one day and not dysphoric the next does not mean that you aren’t really trans.
This Happens Both Ways
 Secret Gamer Girl @SecretGamerGrrl
Secret Gamer Girl @SecretGamerGrrl Worth noting that in the event a confused cis person were to attempt medical transition without being stopped by any of the absurd number of gate keepers and actual medical professionals whose sign-off is typically needed, here's what would happen: They take some pills, or a shot
Secret Gamer Girl @SecretGamerGrrl which will then proceed to make them feel absolutely awful, like pouring sugar into the gas tank of their brain. At which point one assumes they would immediately cease taking the hormone supplements they did not actually need and resume a normal life with no lasting consequence
Secret Gamer Girl @SecretGamerGrrl Should a REALLY stubborn and confused cis person ignore feeling like total garbage and keep on taking HRT they shouldn't be taking for several months, they might also experience some acne and/or their skin clearing up and looking great, and a woman might start growing facial hair
Secret Gamer Girl @SecretGamerGrrl a man in such a position might deal with gynecomastia after like, a year or so, give or take, of again, feeling like complete garbage from taking unneeded estradiol supplements. Anyone, in a similar timeframe, might be looking at their genitals acting like the wrong sort, which
Secret Gamer Girl @SecretGamerGrrl again, I kinda figure is something where one would go "hey this ain't right" and just stop taking the medication they are misusing. Where, again, things would just then go back to normal.
Oh and all of this is me talking about HRT. Usually what bigots are doing is talking about
Secret Gamer Girl @SecretGamerGrrl puberty blockers as if they were HRT. If some confused cis kid takes puberty blockers the grand total of what would actually happen is.. not starting puberty until they realized they were taking them for no particular reason and stopped. No side effects of any sort to worry about
Sometimes you will hear naysayers suggesting that taking hormone therapy always improves mental health. I heard this myself when I came out to my mother. “Estrogen makes everyone happier.” This is flat out false. When cis people are put on cross-hormone therapy it always results in dysphoria. This is one reason why Spironolactone is rarely ever prescribed to men, because the anti-androgen factor causes mental instability. Five to ten percent of cis women suffer from polycystic ovary syndrome (PCOS), a condition which causes the ovaries to produce testosterone instead of estrogen. Ask any one of them how their mental health has been, and they will give you an earful.
One very potent demonstration of this is the tragic case of David Reimer. At seven months of age David and his twin brother were given circumcisions to treat a bad case of phimosis (a skin condition on the foreskin). David’s went horribly wrong, and the penis was destroyed. The decision was made to perform vaginoplasty and raise him as a girl, including estrogen therapy at pubescence. By the age of 13, he was deep into suicidal depression and suffering greatly, as no amount of coaching and encouraging can make a boy enjoy being a girl. When his parents informed him of what had happened, he returned to a male presentation, switched to testosterone therapy, and over the course of his teen years had multiple operations in order to transition back to male.
People know when they’re living the wrong gender.
Psychologist John Money oversaw David’s case and was largely responsible for the decisions that were made in David’s upbringing. Money, seeking to make a name for himself, massively misreported on David’s case, calling it a complete success in his reports. The result of this echoes to this day, as Money’s reports were used as an example of why performing genital corrective surgeries on intersex infants was an appropriate course of action. Fifty years later there are still doctors who believe that you can just change a child’s genitals and raise them as that gender and it will stick.
This is the tragedy of the intersex community. Roughly one in every 60 births results in some kind of intersex condition (though not all of these are related to genitalia). Often times the “corrective” procedures used on intersex children results in a loss of function and/or sensation. Far too frequently, doctors would opt towards forced female assignment because it was easier to construct a vulva than a penis.
Social Dysphoria
Nightling Bug @NightlingBug When you interact with very masculine men, you're nervous. You don't really know how to carry on a conversation with them, or want to. You feel an expectation, from them, to be something you're not. You quietly judge them for being too "bro"-y, "basic."
Nightling Bug @NightlingBug Being vulnerable around strange men is terrifying. You're anxious when you use the public men's room. Changing in a gym locker room is unthinkable. You do not feel ownership of these spaces. You are very concerned about strange men observing you, or your body.
Nightling Bug @NightlingBug You're awkward at social touch. You might crave touch, like most people, but you feel like you're almost entirely incapable of receiving it warmly. When giving a hug, something about your torso feels like it will be *offensive* to others. (Whatever it is, they don't notice.)
Nightling Bug @NightlingBug You can't talk about sex, or attraction, or the bodies of people you're supposed to be attracted to. Even when your commentary is solicited, everything you could say feels unwanted and inappropriate, even if it'd be fine coming from someone else. You freeze up.
Nightling Bug @NightlingBug You struggle even to voice innocent physical compliments to others, like "Looking good!" You are hyper-aware that virtually anything could sound like unwanted sexual attention, coming from you. You feel like your attention is uniquely, universally unwelcome.
Nightling Bug @NightlingBug When an AFAB friend expresses disapproval, you're devastated. You scramble to get their approval back. You're worried you're coming across as a simpering "nice guy," all of whom you despise. You just value your AFAB friends' opinions more highly, for reasons you can't explain.
All social gender dysphoria orbits around one central concept: “What gender do people believe me to be?” Social dysphoria is about how the outside world perceives you, how others address you, and how you are expected to address them. This applies differently prior to the trans person becoming self-aware of their own gender versus how social dysphoria is experienced after a trans awakening (cracking one’s shell).
While still in the dark, the only awareness is that something seems off about the way you interact with your interactions with other people. People of your assigned gender seem to interact with each other in ways that do not feel natural to you. Their behaviors and mannerisms feel strange and surprising, where interactions with individuals of your true gender feel easier. You relate to people closer to your own truth.
For example, an AMAB trans person may find themselves very uncomfortable in groups of men. They may feel out of place and struggle to fit in among their male peers. Masculine social interactions don’t come naturally to them, and trying to emulate their male friends feels awkward. They may feel themselves drawn more to friendships with women, but become frustrated at the social and heterosexual dynamics that come into play between men and women, preventing them from forming platonic relationships. This is if women are willing to form friendships at all. They may find themselves deeply hurt when women shy away from them on principle.
Some non-binary people feel social incongruence in interactions with both men and women, which may persist even if they change their gender presentation.
This feeling of wrongness intensifies as the person becomes more and more aware of their own incongruence, and upon realizing who they really are it takes on a new shape. For binary trans people this often may be about the intense need to be seen as your true gender, be it male or female. Some non-binary people experience this more as euphoria at being seen as neither male or female and thus only being referred to in ungendered ways, or from being read as different genders by different people in the same setting. Some experience intense euphoria when people are incapable of reading their gender and become confused.
Social dysphoria is where pronouns and misgendering come into play; being addressed with a gendered pronoun such as she, he, him, or her which is not the pronoun that aligns with our gender is extremely discomforting. Granted, this is true for all people, including cisgender people, but where a cis person may be insulted by being misgendered, a trans person will feel hurt. It’s like nails on a chalkboard, or steel wool across skin. Hearing the wrong pronoun is a reminder that the person you are talking to does not recognize you for the gender that you are.
Gender-neutral pronouns can also be unsettling for binary trans people if used in a way that make it clear the person is avoiding the pronoun that matches them. This often is an indication that a person has been read as being transgender, and the person addressing them doesn’t know what pronouns they use. Asking their pronouns can resolve this situation immediately, but the paradox is that even in that scenario, having their pronouns asked may itself induce dysphoria around having been recognized as being trans. It is sort of a catch-22.
Singular they can also be used maliciously when a transphobic individual refuses to use the correct pronoun, but knows they will get in trouble for using the wrong pronouns. Tone and intent matter a lot.
The same also applies to names. Being called by one’s given name (deadname) instead of their chosen name can feel invalidating when done ignorantly, and downright dismissive when done intentionally.
It may also manifest as joy or embarrassment at being labeled as your true gender while still living as your assigned gender. Examples:
- An AMAB person being labeled a girl, intending insult, but it causing them to blush rather than get angry.
- An AFAB person being called Sir, and feeling better for it.
 Dr. Emmy Zje @Emmy_Zje
Dr. Emmy Zje @Emmy_Zje The irony in “trans women mimic gender stereotypes” is the only time I DID mimic stereotypes was when I was forced to interact with men. And I did so out of a sense of survival and a longing to try and fit in.
I didn’t transition into stereotypes…I transitioned out of them.
The discomfort caused by social dysphoria can pressure a trans person to act and present in an exaggerated manner in order to try to convince the rest of the world that they really are who they say they are. Transfeminine people may concentrate on makeup and feminine clothes, and become quieter in order to seem more demure, speaking in a higher voice. Transmasculine people will lean on masculine clothing styles, stand taller, suppress displays of emotion, start speaking louder, and make their voices intentionally deeper. Some non-binary people may consciously alter their presentation to be less obviously masculine or feminine, which can resemble the techniques of binary trans people with similar bodies, or may play up intentionally conflicting gender cues.
Physical vs Social Dysphoria
Some physical traits which may cause discomfort all the time for some trans people may only manifest as a social dysphoria for others. For example, some people may only be self conscious about their physical appearance when it causes them to be misgendered or clocked (read as being trans), and feel completely comfortable when interacting in environments where they are always seen and treated as their true gender.
I, myself, have no direct physical dysphoria around my voice; I actually really enjoy singing in my natal baritone, and when I am home with just my family I let my voice relax. When out in public, however, being able to speak in a feminine voice plays a critical role in my being seen as a woman by strangers, so I put a lot of effort into training it into a feminine sound. My feminine voice turns on the instant I answer the phone or leave the house, it isn’t even a conscious thing.
“One of us!”
A very curious and surprisingly common phenomenon is that closeted trans people have a tendency to find each other without ever knowing they’ve done it. There’s a funny pattern that I have heard duplicated over and over where one person in a friend group realizes they are transgender, starts to transition, and that inspires other members of the group to also realize they are trans and come out as well.
 kiva @persenche
kiva @persenche @Whorrorer i can know a cis woman for a year and not feel like i'm all that close to her.
i can know a trans woman for three hours and feel like i've known her my whole life.
Trans people subconsciously tend to gravitate towards each other’s friendships, both out of a need for peers who think and act the same as us without judgments, and due to a kinship of social ostracization. This is not exclusive to trans people, of course, and occurs with all types of queer people, but the way it has a rippling effect is quite powerful. It’s very similar to the way an entire friend group will get married and have kids all in response to one member of the group initiating.
Trans people often continue to self-select their groups post-transition as well, as we simply understand each other better than cis people can. There is an energy that occurs when a group of trans people get together in a location, the room becomes charged with camaraderie and commiseration. We all have so much in common in our histories, so many shared experiences, that (short of personality conflicts) we instantly bond together.
Societal Dysphoria
Gender roles exist, and, as much as we may try to buck them and point out the sexism that exists, there will always be expectations placed on people for their gender. The strongest of these are in marital and parental roles; “Husband”, “Wife”, “Mother”, “Father”, these terms come with loads of baggage attached to them, and the wrong role, or even any role at all, can feel like a lead-lined straitjacket. You are given a whole book full of behaviors and actions, likes and dislikes, that you are just expected to fulfill, and if you fail to meet those requirements then you are seen as a bad spouse or a bad parent. In the case of non-binary people, you may be given competing expectations that are impossible to fulfill, or even be reproached by others for assuming a gendered role at all.
An AFAB parent who gives birth may experience severe dysphoria around being labeled as a mother. The vast majority of resources for birth are extremely female-gendered, so just the very process of conceiving, carrying, and giving birth is exceptionally loaded with gender expectations. If you are pregnant then you are labeled a mom, regardless of how you actually feel about your role, and with that comes a whole load of assumptions — assumptions about caregiving, breastfeeding, and child-rearing.
Cisgender-passing transfeminine individuals also run into this. If you are holding an infant or tending to a child then you are labeled a mom (unless the child is mixed race, in which case you’re demoted to nanny, but that’s a whole other topic). This can be validating, because it is a sign that you’ve been seen as a woman, but it can also be extremely invalidating when cis women start to talk about what they think are shared experiences with reproductive processes.
Some unexpected ways that societal dysphoria can appear are in the need to conform to the social standards of your true gender. For example, many trans women have stories about feeling the need to cover up their chest pre-transition out of an intrinsic sense of modesty. A discomfort at swimming topless is a common trait, even when there is no understanding of one’s true self; something just knows.
Shame
Failure to live up to these roles can manifest intensely as shame and humiliation. Growing up closeted and struggling to fit into common gender tropes often results in signs of disappointment from parents and peers who expected otherwise. A father may be disappointed that their AMAB child isn’t willing to engage in sports or other masculine activities. Female peers may demonstrate disapproval of an AFAB teenager choosing to hang out with a male social circle. Teen boys may ostracize an AMAB trans person who doesn’t join in with their humor.
These kinds of situations can lead to bullying and abuse, pushing the trans person to feel isolated, alone, and out of place. This sense of division then creates feelings of shame for failing to be the person everyone expects them to be. This then manifests as depression on top of other dysphoria, compounding their pain.
Dr. Emmy Zje @Emmy_Zje Guilt is a byproduct of shame, shame is a byproduct of transphobia, and transphobia is a byproduct of lies based in fear.
Once you realize this, you can begin to see “trans” for what it is...a beautiful manifestation of nature. A gift to be cherished, not a curse to be hidden.
The shame becomes especially intense at the moment of revealing themselves to be trans. Transphobic friends and family having negative (sometimes even violent) reactions to a trans person coming out of the closet converts that shame into extreme guilt and disgrace. An adult trans person in a marriage may feel a tremendous amount of remorse at upending their spouse’s life by revealing themselves. They may expect reproach from their neighbors and peers, and fear how that will affect their spouse and/or children.
This too is a form of gender dysphoria, as these influences would not have been felt if the person had been cisgender.
The other way shame comes into play is in the systemic transphobia present in our society. Trans adults of today grew up watching transphobic media in their childhood. The transsexual obsession of the late 80s and early 90s was horrifically traumatic for trans kids of the time, watching all the adults and peers around them laugh and jeer at and be disgusted by people whom they not only identified with but strongly empathized with and looked up to. This shame sits with us for our entire lives; it is a fundamental reason for why so many trans people do not come out until their late 30s or later, because only when they reach mid-life are they able to overcome that shame.
Shame also tends to build up until it boils over into radical action. A very common aspect among trans people’s histories are cycles where they will build up their presentation, fighting their feelings less and less, until suddenly they feel overcome with shame and purge everything, vowing to never pursue those feelings again. This pattern repeats over and over again.
Dating and Romantic Relationships
 Callidora @Adoratrix
Callidora @Adoratrix I get the thinking. Trans girls grow up falsely believing they're guys, and so are assumed/expected/raised to experienced and express normative heterosexual attraction to women. If you're a trans lesbian, you transition, but you're still into women. So it's the same, right? No
Callidora @Adoratrix So let's talk details. To begin with, it's worth pointing out that most trans lesbians don't exactly experience normative heterosexual attraction to women in the same way that cishet men do. Dysphoria and confused gender feelings mess with that a whole lot
Callidora @Adoratrix Before I transitioned, just the thought of doing any sexual or romantic with a girl made me nauseous, because doing that would feel like I was adopting a masculine role - the role of the boyfriend, the male lover - and that kicked my latent dysphoria into overdrive
Callidora @Adoratrix When I first transitioned, my family and friends assumed I was going to be solely or primarily interested in men. Every mainstream cultural message I'd ever absorbed about women (including trans women) told me I needed to be into men
Callidora @Adoratrix Many trans healthcare systems operate on a really really crude system where a cis doctor asks you a bunch of stuff like 'what toys did you play with as a child?' to see if you match up well enough with what a woman is "supposed to be". And women are "supposed to be" into men
Callidora @Adoratrix So, there's a lot of internal and external pressure faced by trans lesbians to disavow their own lesbianism and experience attraction to men. This is nothing like what any straight man experiences, but it is a whole lot like what cis lesbians experience!
Callidora @Adoratrix One last thing is, the way it feels to be a trans lesbian experiencing attraction, sex and romance to other women. It doesn't feel like cishet attraction. It's not burdened by any of those weird, crude expectations. I don't recognize any of that in my life
Callidora @Adoratrix When I read cishet experiences of their sexuality, I feel nothing but alienation. When I read lesbian experiences, they resonate with me deeply and I recongize those things in how I experience my sexuality with the people I love and am attracted to
Societal dysphoria strongly comes into play with courtship rituals. Being forced into being the boyfriend or girlfriend when you are not a boy or a girl is extremely disorienting and often feels very unfair. AMABs may find themselves wishing they were the one being pampered. While unwanted attention causes discomfort for all genders, AFABs may become uncomfortable with even the amount of genuine attention they receive from prospective partners. The expectations placed on them by their partners to fill these courtship roles may feel like a heavy burden to bear. By contrast, dating as your true gender becomes euphoric. Buy a trans girl flowers and see how much she swoons.
A closeted trans person may feel so much pressure to conform to heterosexuality that they suppress their own instincts with regards to relationships and take on a performative role. Many a trans woman has attempted to play the role of a heterosexual husband to a wife, only to realize with transition that they would much prefer the role of the wife. They may not even be attracted to women.
Beyond discomfort, many trans people realize that the dynamics of relationships that they have experienced simply did not fit the shape of how they appeared. Many trans people come to realize after transition that they had never actually dated like a cis person of their assigned gender, instead always having romantic relationships that fit their true orientation. Male to male and female to female relationships have completely different patterns from heterosexual relationships; different courtship rituals, different perceptions, different communication styles. Men relate differently to men than they do to women, and women to women differently than they do to men, even when they don’t know they are men or women.
For example, I myself realized after coming out to my wife that all of my previous dating attempts had absolutely been sapphic in nature. My first order had always been to become good friends with them. Dates would never be labeled as dates because we would just sit and talk somewhere, hanging out together. Consequently, several of my relationships ended simply because I was too scared to make the first move out of destroying the friendship. I would spend half my waking day thinking about them and wanting to be around them, not out of sexual lust, but out of personal infatuation. My first girlfriend straight up told me on our first date that I was unlike any man she’d ever dated because I enjoyed talking instead of just trying to get physical. She broke up with me two months later because I wasn’t as assertive as she wanted from a partner.
These dynamics get even more complex for non-binary people, some of whom can at best describe their dating style as queer. Some struggle to identify what role they play in a relationship. Others take a specific role that is typically seen as a binary gendered role, and may not be the one assumed from their appearance. Some non-binary people wish to be seen as a boyfriend/girlfriend even if they are not a boy/girl. Some want to play a role seen by society as neutral or consisting of aspects from both binary roles. Some non-binary people may feel uneasy about heterosexual dating dynamics in particular, whether they play the “male” or “female” role.
As many people define their orientations in terms of their gender relation to men and women in a way that does not map to non-binary people, some non-binary people may find the traditional language of “heterosexual” or “homosexual” itself induces dysphoria.
Sexual Dysphoria
Closely related to societal dysphoria is dysphoria centered around sexuality, sexual relationships, and the act of having sex. Heteronormative gender roles come loaded with the expectation that AMABs will top and AFABs will bottom. These dynamics get reinforced by our popular media, by toxic masculinity, and especially by our pornography, even in transgender pornography. (The bulk of trans/cis pornography involves trans women topping, etc.) Deviations from these roles often result in shame, both from partners and from peers.
Of course, this is not an absolute by any means, and many heterosexual cis couples do find ways out of these molds, finding a new dynamic in their relationship, or engaging in kinks to satisfy desires. Some couples find they aren’t sexually compatible at all and seek other partners. However, there are many, many external pressures discouraging this kind of self-awareness and discovery, and breaking away from those demands can be extremely difficult — even traumatic. This is particularly true when there is a background of conservatism or religious virtuism.
Cisgender gay relationships shirk this by virtue of necessity, opening the doors for individuals to explore what role leaves them more fulfilled. Some gay couples have an established dominant/submissive dynamic, and they enter into the relationship with that already understood. Others resolve it by switching up which partner is dominant. Yet, gay relationships can still get caught up in these kinds of expectations in regards to butch/femme, bear, and twink dynamics.
What does all this mean? Trans people who enter into perceptually heterosexual relationships pre-transition sometimes find themselves losing interest in sexual intercourse, as penetrative acts do not produce the fulfillment that they would expect. In extreme cases it can feel completely wrong and trigger panic. The sensations may feel pleasurable, but the experience is out of place, and the act itself feels forced.
Kathryn Gibes @TransSalamander Did any other trans girls get to the point pre-transition where they had to basically dissociate in order to top or was that just me lol
This can lead to one feeling less enthusiastic or even disinterested in sex, as half of what makes up sex drive is the mental context of the situation. Many trans people never even experience sex until adulthood, functionally operating as sex-averse due to how severely their dysphoria has shut down all sex drive. They may still perform for the sake of their partners, but not get as much enjoyment as they could, and even end up disconnecting from reality around them in order to accomplish the task.
This dysphoria may be so significant that they find themselves taking a sexual identity that they don’t actually connect with. It is not unheard of for a trans person to realize after coming out that they never actually felt a connection to the sexual orientation that they had identified with previously, but were instead using it as a way to feel less dysphoric in their sex lives.
Some trans women, for example, identified as gay men pre-transition out of a desire to have a partner that treats them like women during sex, but find themselves to actually be lesbians once that demand is lifted. Others may attempt to live as gay men, but find that the role doesn’t fulfill them because they know their partners see them as men.
The Coercive Male Gaze
Author's Note: This specific type of sexual dysphoria is difficult to explain in generalist terms, so I am going to take a departure here and write about this from my own personal experience. The following is presented from my perspective as a binary trans woman. As such, this may not be completely relatable to all trans people. My apologies.
 "Swole Mom" - How Baby, by Lindsay Ishihiro
"Swole Mom" - How Baby, by Lindsay Ishihiro There is a saying that is very well known in sapphic circles: “Do I want to be her, or be with her?”
It can be hard to tell the difference between sexual attraction and envy, especially when you’re a closeted trans teenager. Our entire society is built upon heterosexuality; it is simply the cultural default, to the point that even prepubescent children are barraged with messages about male to female attraction. Consequently, interest in aspects of the lives of the “opposite” sex is almost always immediately perceived as being sexual attraction.
What is the result of this? Usually… shame. Trans children often internalize their view of their peers based on their true gender, and one does not objectify their equals. Thus the child is motivated to hide those interests out of a desire to not be seen engaging in that kind of sexual objectification. This is even further compounded if the child has been raised in a setting with very strict moral codes, such as in a conservative religious upbringing.
Growing up as a closeted trans teen in an evangelical Christian household, I knew that if I was ever caught looking at women in what was seen as a sexual manner, I would be punished. I knew if I was ever found handling women’s apparel, there would be a lot of very awkward questions which I was not prepared to answer. This posed a very serious problem for me, as someone with a strong fascination with women’s apparel, particularly lingerie.
There is a Simpsons clip where Moe Szyslak is put on a lie detector test, and by the end of the test he has confessed that he will be spending the night ogling the women in the intimates section of the Sears catalog. The entire crux of the scene, and the source of the comedy, is the shame that is cast on Moe for engaging in this desperate act of objectification. I grew up knowing that this is how I would be perceived for my interest in women’s clothing.
Out of shame and fear, I did everything I could to hide this passion, because I simply could not bear for someone to view me like the teenage boys who masturbate to any material they get their hands on. What made this fear even worse was that I also believed that my interest was sexual.
When you see the world through a duck shaped lens, everything looks vaguely like a duck. The only framework I had been given to understand my interest in women was through sexual desire, and thus every feminine interest I had became warped into a sexual desire. My wish to be a bride morphed into a bridal kink, my desire to have a child warped into an interest in pregnancy porn, and my own need to be a girl was redirected into a transformation fetish.
But on top of all of this, I was terrified to be seen expressing legitimate sexual interest in other women. I had male friends who were notorious rubberneckers and slack-jawed gawkers; one of my former employers had an awful habit of leering at attractive women when we were out to lunch, which made me very uncomfortable to be seen with him.
I could not stand to be associated with that male gaze. Even around the most beautiful women, I would avoid even looking at them, because I did not want to be seen as the kind of person that stares at women. I did not want to be seen as a predator.
This is the coercive male gaze: compulsory heterosexuality placed upon closeted trans women due to heteronormative ideologies — a cognitive dissonance that causes intense guilt and shame surrounding appreciation of one’s peers and gendered interests.
Once you remove this male framework – once one is able to perceive themselves as female and accept these interests and observations as valid – that shame and guilt completely evaporates. Even when the interest is sapphic in nature and genuinely includes sexual desire, it is no longer tainted with this layer of objectification. I am able to appreciate the femininity and the beauty of my female peers without judgment, and I can compliment them without fearing being perceived as a creep or having my intentions misinterpreted.
It was a dysphoria I could not possibly have put into words until after it had finally been relieved. I was even more relieved as I began to integrate into queer women’s spaces and came to realize that women are exactly as thirsty as men are; we’re just (usually) much more respectful about it. It was a release of guilt that I didn’t even know I was carrying.
Presentational Dysphoria
Clothes. Hair. Makeup. Jewelry. Glasses. Piercings and other body modifications. Even personal hygiene can be a factor of presentation, such as the shaving of body hair or how you take care of your skin. All of these things are gendered in society, clothing and hair especially.
While the sexual revolution of the 1960s and the business fashion craze of the 80s did wonders for blurring the gap between masculine and feminine presentation (largely by normalizing masc fashion as androgynous), there are still enormous pressures to conform to traditional gender norms. Gender non-conforming dress is so instantly marked as queer that any time a woman wears a tailored suit she is marked as a lesbian, and a dad who puts on an Elsa costume because his son wants to have a Frozen party is labeled as subversive and abusing his child.
Long hair on men has been seen as an act of rocker rebellion for decades, and men with long hair get discriminated against as being layabouts and bums. Short hair on women is often read as queer or butch (unless they’re old, then it’s expected), and women are often pressured to keep their hair long. Pierced ears on men became somewhat more normalized in the 90s, but are still seen as an act of rebellion, and some employers won’t allow men to wear earrings. Makeup on men is so stigmatized by toxic masculinity that even men who like makeup feel pressured to avoid it.
Like it or not, presentation is gendered, and it is extremely common for trans people to want to present themselves in the fashion of their true gender, and a desire to be free of the shackles of gendered presentation is common among all trans people, regardless of where they sit on the gender spectrum. For AMAB individuals they may manifest as a wish to incorporate more feminine elements; for AFABs it may manifest as a want for a more masculine appearance. This may come as a full push towards the opposite of their assigned gender, or a desire to seek a middle-ground in pursuit of androgyny. It may even simply be a wish to not present as your assigned gender.
Not all transfems present feminine, not all transmascs present masculine, and not all non-binary people seek androgyny. Butch AMAB trans people are valid; femme AFAB trans people are valid. Presentation is not gender; gender is not presentation.
Presentational dysphoria typically appears early on in the form of a fascination with the styling of another gender, and a wish to be able to present as people of that gender do. That desire may be fulfilled somewhat by seeking out styling that is unisex, but typically that wish is self-gatekept by statements of “I’m not confident enough to attempt that.” AMABs often run into issue here where this desire often gets trapped behind heteronormative expectations, causing an interest in feminine presentation to be misinterpreted as sexual desire.
Post-transition presentational dysphoria is usually simply a case of high discomfort when attempting to present as one’s assigned gender. It may not even be about how one looks, but just the way the clothing makes you feel. For the first year and a half of my own transition I could not bear to wear unisex t-shirts because they just made me feel more masculine. Even now I have to cut the collars out of them because the close neck makes me feel dysphoric.
Presentation’s Effect on Physical Dysphoria.
Nightling Bug @NightlingBug When you get ready to go, you just roll out of bed and throw on whatever. You don't really do any self-grooming, or care about what's on your body. You're a little proud of your lack of vanity, your deeper, non-appearance-level existence.
Nightling Bug @NightlingBug Your clothes are chosen almost entirely for comfort. And for you, comfortable means loose and baggy. You can't stand wearing clothes (that others claim are flattering!) that are close-fitting in the wrong places, that draw your own attention to certain parts of your body.
Nightling Bug @NightlingBug Clothes shopping for yourself is a hassle at best and a source of stress and anxiety at worst. When you do find clothes that fit and look okay, they don't make you *happy*. You don't feel more confident in them. You're just relieved you can go home.
Nightling Bug @NightlingBug Occasions where you *must* dress up, like weddings and funerals and job interviews, are the worst. Even after all of the grooming and wardrobing, you feel self-conscious and awkward in formalwear. It makes you feel *fake,* like a lump of sludge pretending to be a fancy person.
Clothing can also play a major role in the level of physical dysphoria a person experiences. Men’s clothing is always cut very boxy, straight up and down on the vertical and very square in the horizontal. Women’s clothing is cut for more curves, accentuating waistlines and hip shape. Men’s pants feature a lower crotch to make room for external genitals, and no fitting for curves, where women’s bottoms are the opposite. Women’s clothing is often form fitting, where men’s clothing is rarely form fitting at all. Men’s clothing is often made of sturdier and thicker materials, meant to be worn as a single layer. Women’s clothing is often made of thinner and stretchier materials, expected to be layered together.
Because these structures are meant to fit the masculine or feminine forms, they tend to amplify the sensation of wrongness. A classic effect is the way that the difference between men’s and women’s jeans can have a radical effect on a trans person’s comfort level. Unfortunately this works both ways, as even affirming clothing can reveal how your shape is a mismatch.
I, myself, am very feminine in my preferred presentation, and I’ve had a longing to wear dresses from when I was just five years old. I abhorred wearing suits, hating the way they fit on my body, since they always tugged in ways that felt very incorrect for what my body needed. I refused to wear any denim for most of my life because men’s jeans always felt so incorrect (women’s jeans and leggings, however, feel amazing). Then as I entered into transition and began to present more female, my dysphoria struck again in the ways my body did not conform to what women’s clothing was expecting (too much in the crotch, too wide and bulky in the shoulders, too large in the waist, not large enough in the chest). It wasn’t until the second year that I had experienced enough change in my shape to where women’s clothing was properly affirming of my shape.
What does this look like? Well, it looks a lot like other common body image issues: a tendency to avoid anything form fitting, leaning towards softer fabrics and baggier clothes. A classic gender dysphoria trope is the kid who wears nothing but sweatpants and hoodies. Clothes will be oversized in order to keep them from hugging the body. AFABs may prefer to wear compressing sports bras in order to minimize their chests, and avoid anything with a tight waistline.
 Cherry Blossom @DameKraft
Cherry Blossom @DameKraft Feeling envious of other girls for being pretty is a thing that many many women feel. Dysphoria is a real headfuck of a layer on top of that feeling, yet I just wanna say that if you’re a trans woman feeling envious of another trans woman, that’s you being a actual woman.
Internally it most often manifests as intense jealousy of the people you wish you could be: jealousy over an influencer’s body shape, a strong desire for the outfit of a person on the street, and most especially envy of other trans people. This feeling often persists well into transition, because this sensation of wanting to be other people of your gender is actually completely natural, even for cis people.
Presentation’s Effect on Social Dysphoria.
Presentation can be important for avoiding misgendering, especially early in transition. A lot of trans people feel a need to perform their gender in order to be accepted for who they are, leaning in to feminine or masculine presentation more than they actually would like in order to make up for their body and ensure that people gender them correctly. Those pursuing medical transition may find this need becomes less important as their bodies change and they become able to be gendered correctly without all of the performance.
Performative presentation was practically required prior to the reformation of WPATH in 2011; anyone who showed up to a doctors appointment without extreme feminine or masculine presentation risked be labeled a fake and losing their treatment under the Harry Benjamin Scale. Trans women actually would lose their estrogen simply for wearing jeans and a blouse instead of a dress, or for not putting on enough makeup. This is one of the reasons why transmedicalist ideology is so dangerous: it would see us returning to this system, labeling anyone who doesn’t meet stereotypical views of femininity and masculinity as not actually transgender.
Presentation is especially important among prepubescent children, as they lack any significant secondary sexual characteristics. Clothing and hair are the only ways we have to show the gender of a child, so much so that if a baby simply wears a pink shirt, strangers assume it is a girl. Even unisex clothing for kids is strongly gendered by way of colors and graphics. For trans children, it can be extremely distressing to be either forced to cut their hair or required to grow it out. Denying dresses to a trans girl or transfeminine non-binary child, or forcing them onto a trans boy or transmasculine non-binary child, can be debilitating to their morale.
Existential Dysphoria
When you grow up as the wrong assigned gender, you are going to miss out on a lot of things that should have been available to you if only people had known. Sleepovers, camping trips, girl/boy scouts, shopping trips, cheerleading or sports. Events that are co-ed may have very different feelings attached to them based on how you engage with them, like going to prom, religious ceremonies (such as having a bat mitzvah instead of a bar mitzvah), and even just the act of courtship. This dysphoria may also be biological in origin, such as a sorrow over having not given birth to or breastfed your children.
These missed opportunities can manifest as feelings of loss and hurt. Furthermore, the memories of things you did have access to but wouldn’t have otherwise, or events that were performed in the wrong gender, can also be a sour point, as these may have awkward attachments. Imagine having to be a groom at your wedding when you know you should have been a bride; growing up dreaming about your perfect wedding, and then playing the wrong role in it.
Sometimes existential dysphoria can manifest existentially, hitting you with all the grief of the youth lost. All the dating, the teenage antics, the parties, even just having been able to be sexual with the correct parts while your body was young and you had no responsibilities. It is time that can never be gained back.
Many trans people attempt to recapture some of these lost events, hosting or attending queer proms, organizing sleepovers, performing vow renewals with their spouses, and engaging in common puberty rites of passage like having a mother figure help them shop for their first bra, or having a father figure teach them to shave. However, ultimately, existential dysphoria is something that can never be relieved. You can make new experiences to replace the ones you lost, but you can never turn back the clock.
This is one of many reasons why affirming trans youth is so important. Boys want to do common boy things, girls want to do common girl things, and non-binary children want to do whatever feels correct to them, and when they miss out they will not forget.
Managed Dysphoria
Growing up in the closet, even when you don’t know you’re in the closet, becomes an existence built on top of coping mechanisms intended to alleviate dysphoria. The following are ways a closeted trans person may find to alleviate the dysphoria they experience in their day to day lives:
-
When a video game gives you the option of choosing your gender, you tend to choose differently than your assigned gender. This may be accompanied with excuses to defend that choice. “It defaulted to male and I didn’t care.” “I don’t want to stare at a guy’s butt for hours.”
-
A preference for literature and film with characters of your true gender, or with characters who break gender norms (Mulan, Little Women).
-
Pornographic outlets which satisfy strong desires or feel more relatable, such as a draw towards gay/lesbian porn, bridal kink, or transformation sequences.
-
Crossdressing or performing drag.
-
Finding excuses to cut hair short, or to grow it out.
-
Shaving of body hair, or a refusal to shave hair you’re expected to.
-
Wearing loose and baggy clothing that hides the shape of your body.
-
Avoiding social gatherings whenever possible, seeking isolation.
-
Becoming intimately educated about some gender-associated topic, such as men’s or women’s clothing design.
-
Obsessively working out (AFABs).
-
Helping cis partners to shop in order to live vicariously through their presentation.
Nightling Bug @NightlingBug You're worried that you might be homophobic, even though you believe in gay rights, because "LGBT+ stuff" fills you with a deep discomfort. It all seems so flamboyant and overtly sexual. It makes you want to shrink down and disappear, before you die of secondhand embarrassment.
Nightling Bug @NightlingBug Later, when you meet real queer people, or your friends come out of the closet, you start to idolize them. But you're also jealous. They're *free* and *real* in a way that seems impossible for straight people, like you. They have huge, *real person* worries and desires and lives.
Because so much abuse is handed down onto gender non-conforming children, many trans people grow up learning to hide their natural personalities out of sheer necessity. Many trans people speak about having a phase of life where they attempted to “buy-in” on their assigned gender, performing masculinity or femininity to extremes in order to try to “fix” themselves. This leads to repression tendencies which may even superficially appear toxic, but are simply the results of trying to hide every scrap of their true selves.
-
Growing and meticulously grooming facial hair (the so-called “denial beard”).
-
Taking up makeup artistry in order to perfect a high femme look.
-
Presenting extremely masculine or hyper feminine.
-
Avoiding any conversation about fashion for any gender. Dissociating whenever fashion conversations or activities occur.
-
Obsessively working out (AMABs).
-
Assuming a strongly stereotyped gender role in a relationship (e.g. the dutifully modest housewife).
-
Marrying and having kids in anticipation that it will “fix” what’s wrong with you.
-
Buying in to ultra-conservative attitudes towards gender and sexuality.
-
Expressing homophobia and transphobia in self-defense to ward off suspicion.
-
Aggressively-passive engagement in anything connected to one’s true gender.
Finally, another very common coping mechanism is to find means of escape or mental engagement in order to forget your own feelings.
-
Intensely investing large amounts of time into hobbies.
-
Long hours spent at work.
-
Chain-binging movies, TV shows, or books.
-
Spending all idle time playing video games or on social media.
-
Obsessively cleaning one’s living space.
-
Sleeping. Lots and lots of sleeping.
-
Drug and alcohol use.
Impostor Syndrome
Impostor syndrome (also known as impostor phenomenon, impostorism, fraud syndrome, or the impostor experience) is a psychological pattern in which an individual doubts their accomplishments and has a persistent internalized fear of being exposed as a “fraud”.
Society in general is very good about making trans people doubt themselves. We receive tons and tons of subliminal messages through out our lives saying that being trans isn’t normal and that anyone who is has to be exceptionally special. Cis media’s obsession with the “born in the wrong body” narrative has led to a lot of false information being internalized by trans youth. Many, many trans kids grow up thinking they aren’t actually trans because they don’t know that they are a different gender but simply wish they were. Many non-binary children grow up knowing something is wrong, but not believing they’re trans because they don’t feel like a binary trans person.
On top of this, messages saying that trans people hate their bodies or hate their genitalia have polluted the awareness landscape, so that many people who either do not experience physical dysphoria (or simply think theirs isn’t very strong) go around believing they aren’t “trans enough”.
 Faith @RoseOfWindsong
Faith @RoseOfWindsong Gay people 2 decades ago: *exist*
Bigots: "They're trying to turn our children gay! We must protect our children!"
Trans people now: *exist*
Bigots: "They're trying to convince our gay kids they're the wrong gender! We must protect our gay children!"
On top of this, the constant messaging from transphobic media that trans people are not actually their true genders and are simply trying to trick people into believing otherwise gets internalized like a virus. This creates a lot of self doubt about the authenticity of one’s gender, especially in the face of so many gender stereotypes. Seeing oneself fail to meet those stereotypes can make it very easy to convince yourself that you do not live up to your own gender (note: cis men and women get this too, far too often).
Furthermore, due to a history of transphobic abuse, many trans people suffer from damaged self-esteems, and often already have difficulty with self-doubt. Gender dysphoria also causes depression, which further contributes to and reinforces those doubts. This all leads into a massive cluster of self-invalidation that can lead someone to struggle over and over again to accept their own gender identity.
But here’s the thing… only trans people are worried about if they are actually transgender! A cisgender person does not have this obsession with their identity: they think about it, they process it, they move on. If you keep returning to these thoughts over and over again, this is your brain telling you that you took a wrong turn.
The world is full of influences put in place to fill us with doubt and keep us from breaking outside of the established social order. These are some of the systems and ideologies that seek to invalidate trans people and keep us from self-actualizing.
Autogynephilia
 𝓙𝓸𝓬𝓮𝓵𝔂𝓷
𝓙𝓸𝓬𝓮𝓵𝔂𝓷  ⚢
⚢
 @TwippingVanilla
@TwippingVanilla A friend of mine who just started her transition this week asked me yesterday if I ever got turned on by seeing myself. I knew immediately what she was actually asking, so this is a PSA for all those trans femmes out there feeling invalidated by their own bodies.
𝓙𝓸𝓬𝓮𝓵𝔂𝓷 ⚢ @TwippingVanilla Im gonna be blunt: Your gender is not invalid because you get an erection when seeing yourself dressed as feminine. We’ve all gotten it. It doesn’t mean you’re fetishizing. It doesn’t mean you’re not actually trans.
All it means is that you feel good about how you look.
𝓙𝓸𝓬𝓮𝓵𝔂𝓷 ⚢ @TwippingVanilla Gender Euphoria is sexy. Being comfortable in your clothes is sexy. Liking the way you look is sexy. *Feeling sexy is sexy!!*
That triggers a turn on, the body reacts to sexy things.
Here’s the kicker: Cis Women get this too!!! It’s literally just a lady boner!
𝓙𝓸𝓬𝓮𝓵𝔂𝓷 ⚢ @TwippingVanilla Over time this reaction happens less and less as you get more used to preseting as yourself. Eventually most clothes are just clothes, it’s just your new normal.
𝓙𝓸𝓬𝓮𝓵𝔂𝓷 ⚢ @TwippingVanilla But that special outfit that makes you feel really hot? That new dress that you try on for the first time and feel really cute in? That lingerie that you bought specifically to feel sexy in?
Yes, that triggers it. All it means is thst you’re happy.
𝓙𝓸𝓬𝓮𝓵𝔂𝓷 ⚢ @TwippingVanilla Let me tell you, the massive relief my friend displayed at learning that this was completely normal was palpable. The poor girl had been stressing about that so hard.
She didn’t even know about AGP, but she knew the stigmas and was terrified that this meant she was fake.
This pattern was strongly reinforced during the late 1980s when the autogynephelia (AGP) theory of Ray Blanchard gained a lot of traction as trans awareness was just starting to escalate. AGP is a pseudo-scientific explanation intended to “explain” the source of trans women’s identities using paraphilias. Blanchard separated trans women according to if they were attracted to men or to women, while simultaneously invalidating their womanhood. His work completely ignored transgender men, and he dismisses non-binary identities outright.
Autogynephelia attests that straight trans women are actually just gay men who seek a feminine appearance to draw desire from straight men, and that trans lesbians are actually straight men who have become so obsessed with their desire for women that they wish to become a woman in order to gain sexual gratification from themselves.
Blanchard’s theory largely hinged on the way that presenting feminine often resulted in sexual arousal within newly transitioning women. You see, most of his study subjects were patients who were trying to seek hormone therapy for the first time, and as such were still very new to presenting female.
Yes, it boggles the mind, but this was actually considered a valid theory of psychology for years. It even appeared in college textbooks. Blanchard’s research studies did not meet scientific rigor, and his data was found to be extremely flawed (he manipulated his patients, and simply just threw out any data that didn’t fit his hypothesis). A lot of his theories are based in misogynistic views of womanhood, and the man never actually involved any cisgender women in his study to function as a control group. You can read more about how flawed the theory is in Julia Serano’s excellent essay The Case Against Autogynephilia.
AGP had been thoroughly dismissed by modern psychology by the late 2000s, but the damage has been done. In the public’s eye, trans women were all perverted fetishists. Media portrayals of trans women mirrored this attitude, further spreading negative imagery into the public consciousness.
Transfeminine individuals then internalize these messages, and come to the conclusion that they are not actually transgender — just fetishists. It happened to me, and it’s happened to nearly every millennial trans woman I know who figured themselves out as a teen.
You are not a fetishist. The feeling you get from thinking of yourself as a woman is gender euphoria.
Patriarchal Oppression
A common source of invalidation for AFABs is the conflation of gender with the systemic oppression of women, particularly among non-medically-transitioning non-binary people. The message of “oh you just don’t want to be a woman because of how women are treated” is far too often heard, and it can deeply infest your subconscious to the point of self-doubt. But this doesn’t make much sense, because if you’re AFAB and not a woman, that makes you transgender, and, on average, society treats transgender folks worse than women. So transitioning to escape systemic oppression is a dumb concept (and I personally have never met a trans person who has done this).
Radical feminism’s messaging of abandoning female gender roles can also make parsing your own feelings harder. “Am I actually non-binary, or am I just a feminist?” “Am I actually a man, or am I just a very butch lesbian?”. For this, I encourage you to talk to cis woman feminists, especially lesbians. They’ll complain about systems of oppression and the patriarchy, but the problems are all external, and they want to be women. Even very butch lesbians want to be women, just in a different way from mainstream femininity.
Then you have the problem of people believing that to be non-binary is to be androgynous, and to be androgynous is to be less feminine. Feminine enbies are valid! It is okay if you do not want to remove your breasts. It is okay if you enjoy your curves. It is okay if you do not mind being called “she” and “her”. That does not make you any less transgender.
If you feel like you are not a binary woman, then you are not a binary woman. Cis women do not experience that detachment.
Toxic Masculinity
Male-assigned kids grow up positively drenched in messaging of what it is to “be a man”. There are so few examples of positive masculinity in popular media, and AMAB masculine enbies are also so commonly erased in trans representation that being a genderqueer male can feel very lonely. AMAB enbies are often either grouped in with gay cis men or treated like trans women.
You can just be genderqueer! Your identity is valid!
Transmedicalism
This one hits everybody. Transmedicalism (aka Truetrans) is a transgender ideology derived from the Harry Benjamin scale (ranks 5 and 6). It seeks to reinforce the pre-WPATH rules, requiring intense physical dysphoria, demanding medical transition, and often invalidating all non-binary identities. At its core, transmedicalism is a supremacist concept, elevating binary trans people above the needs of any other gender identity, and is a push back against the expansion of the transgender identity. They wish for more gatekeeping than we have today, rail against enbies using the transgender label, and would prefer to see fewer people receive treatment for their gender dysphoria.
To put it succinctly, many transmedicalists hate that the newer generation “has it so easy,” despite the fact that many of their ranks are part of that generation. This ideology started among disgruntled trans elders, but has since spread to other binary individuals, particularly among young trans men.
If a trans person’s first exposure to transness is a transmedicalist, this can severely set back their own self-acceptance and push them even further into the closet. Transmeds are well known to actually tell people “No, you are not trans.”
Do not believe these lies. They are bully tactics explicitly designed to gaslight and dismiss people’s pain for self-gratification.
There are related hurtful concepts a trans person can internalize, revolving around seeing transition as a list of required actions. One such idea is a belief that a person shouldn’t expect being gendered correctly or even complain about misgendering as long as they haven’t changed their gender marker. In other words, legally conditioned pronoun respect, or translegalism. Not only can changing gender marker be a complicated, prolonged process, not only can some people not afford to out themselves by pursuing it, but most countries wouldn’t even allow a gender marker outside of the gender binary. Translegalism convinces a person that they deserve misgendering because of their ID.
Trans-Exclusionary Reactionary Feminism / Gender Critical Movement / Gender Essentialism
Gender Essentialism is the belief that there are innate attributes to a person’s existence that are derived based on what sex organs the person is born with. TERF and GC ideology was born out of the lesbian separatist movement of second wave feminism and fully denies the existence of transgender biology and non-binary identities. The movement has been largely overtaken by right-wing reactionaries, racists, and homophobes, and is now being bolstered by evangelical Christian organizations.
These people will stop at nothing to invalidate your existence. Do not give them the time of day.
Gender Abolitionism / Postgenderism
Postgenderism is a transhumanist philosophy originating in radical feminism which states that gender causes more harm than good, and seeks to eradicate it from our society. Old-school TERFs latched on to GA as reasoning for why trans people should not exist. This trans-exclusionary faction of gender abolitionism believes that all gender is a construct and that anyone who feels strongly connected to a binary gender is either nefariously propagating gender stereotypes or ignorantly following systemic indoctrination. They do not believe in the existence of gender dysphoria, and will attempt to invalidate those who experience it.
Note, this is NOT about trans people who identify as postgender or gender abolitionism as a whole. This is specifically about TERF abuse of the concepts.
Curator's Note: The following page comes from a fantastic post written by Cassie LaBelle and has been reshared with permission. You can read more of her writing on Medium.
Am I Trans?
Long before I started questioning my gender, I had this idle fantasy where one of my best lady friends would walk up to me and say, “Give it up. You’re not fooling anyone.”
If you’d confronted me about this fantasy at the time, I couldn’t have told you what, exactly, I meant by “you’re not fooling anyone.” Deep down I knew that it was probably related to gender, but my lips wouldn’t have been able to form those words. All I knew was that I was pretending to be someone I was not, in some vague, passive, and ephemeral way.
Once I self-accepted as a trans woman and started the long process of coming out, all I wanted was for someone to tell me that they already knew. “I’m so happy you figured it out,” I wanted them to gush. “I’ve known the truth for years. It was so obvious. I don’t know how anyone could have ever thought that you were a boy. I’m so happy that you’ll finally get to live as your true self now.”
Nobody ever said this to me, though. My coming-out process was successful, and most of my friends were supportive, but I never got the external validation that I craved. My friends and family accepted me as trans because I told them I was trans. They hadn’t noticed that I’d spent the past two decades wearing the ill-fitting costume of a man who barely existed.
My good friend Lily coined the phrase “Egg Prime Directive” to describe the fact that trans people have an unspoken agreement not to tell people who are questioning their gender whether or not they are trans.
When someone is just told they are trans, that opens ground for denial; it activates defense mechanisms built by internalized transphobia, and it has a high probability of pushing them further into the closet, if not making them outright transphobic. Even when it doesn’t, it leaves ground for their own subconscious to reject their dysphoria, claiming that they were just manipulated or deceived. The much more effective strategy is to talk about your own experiences with dysphoria so that they see the common grounds and come to their own conclusion about their gender. The code doesn’t forbid helping them to explore their gender; it forbids assigning a gender to them. Or, to put it more succinctly, no one can be told what the Matrix is. You have to see it for yourself.
I’m sure there are some trans people out there who don’t follow the Egg Prime Directive, but I haven’t met them. It’s one of the only things that seems to unify the whole trans community, myself included. Even though I wanted my own external validation more than anything, I now see that true acceptance could have only come from within. The only person who can tell you that you are trans is yourself.
The paradox is that most closeted trans people are absolutely terrible at trusting their inner voice. When you spend your whole life with a nagging disconnect between how the world sees you and how you see yourself, it becomes easier to rely on other people to tell you “who you really are.” Even if you know deep down that all the people in your life are missing some fundamental fact about your identity, it’s nearly impossible to avoid listening to others over oneself.
My goal today, then, is to give you some of the information and mental framing that helped me self-accept. I can’t tell you whether or not you are transgender, but I can point you down a path that you might be able to travel down yourself. I can’t provide the answers, but I can try to give you the right questions.
It is never safe to simply tell someone that they are transgender when they haven’t asked themselves, even when you are 100% certain that they are. You can educate them on gender dysphoria and you can show them parallels between their feelings and your feelings, but you cannot simply say to a person, “You are transgender”.
Why? Because most of the time they won’t believe you.
Internalized transphobia has indoctrinated us all to believe that it’s impossible that we are trans, or that being trans is something negative and reviled. Pressures from within a person’s family or from their upbringing can make it extremely hard to accept themselves.
Trying to tell someone who isn’t already questioning that you think they’re transgender triggers a self-defense mechanism; their subconscious actively tries to reject the statement, and there is a high probability that the suggestion will not only push them further into the closet, but can even make them hostile towards you for making it. Many transphobes show clear evidence of fighting their own struggles with gender, and there is no shortage of trans people who have a history of being transphobic out of self-preservation.
Even when the person accepts your declaration, the fact that you told them instead of letting them discover it themselves leaves an opening for their own self-conscious to instill doubt about their dysphoria and believe that the idea was suggestive, or that they were manipulated into believing they were trans. The only safe pathway forward for someone to learn they are trans is to realize it on their own.
Finally, the entire purpose of being trans is self-assignment and self-actualization. Telling a person that they are trans is surely as coercive an assignment as what was done when they were born. If you want to help them figure themselves out, tell them about your life, tell them how dysphoria works, send them to this site, and give them ways to see how what they experience isn’t something that cis people live with.
Unless, of course, they ask you if you think they’re trans… then the prime directive no longer applies.
As always, please understand that I have no professional training in gender therapy. I am simply writing this from my own amateur research and personal experiences — mostly my own journey and conversations I’ve had with other trans women and gender questioners. Keep in mind that I am coming at this from the perspective of a fairly binary trans lady who transitioned in her early thirties, which means that I am still blind to a lot of the trans experience. Things are different for trans-masculine and non-binary people, as well as for many other trans women. This is not meant to be a universal expert guide — it’s just the best I can give you right now.
Consider That Most Cis People Don’t Think About Their Gender Very Much
If you’re already at the stage where you are questioning your gender — even if that just means looking up “Am I Trans?” and then slamming your laptop shut before you get a search result — congratulations, you’ve already thought about your gender more than most cis people will in their entire lifetimes.
I’ve asked many of my cis friends if they’ve ever seriously thought about their gender identity, and nine times out of ten they have not. Cis people don’t constantly wonder what it would be like to be a girl. They haven’t had daydreams about how nice it would be if they woke up in a different body. Their hearts don’t race when they think about body-swap movies. Some of them may have imagined what it would be like to be in a body with a gender other than their assigned gender at birth, but those thought experiments have been brief and purely intellectual.
There’s no energy there. Not for them. If you feel a weird kind of energy when you think about gender, that probably means something.
Consider That Most Cis People Actively Like Being The Gender They Were Assigned At Birth
This was hard for me to believe at first, but cis people actually enjoy their gender! Cis men like being men, and cis women like being women. They don’t secretly wish they had been born a member of the “opposite” gender or a genderless being or anything else, really. As we’ve already established, they don’t think about their gender much at all.
There are complications here, of course. Plenty of cis men find toxic masculinity stifling and awful, choosing to actively reject the problematic social aspects of their gender. Plenty of women are deeply frustrated by misogyny, the patriarchy, and the tyranny of classical gender roles. “Enjoying being a man” does not necessarily mean loving having to bottle up your emotions in all non-NFL situations, and “enjoying being a woman” rarely means that you love getting belittled by your male co-workers or being constantly asked, “So, when are you getting married?”
Once you cut through all of that, though? Cis people still enjoy their genders. They might wish that certain aspects of how their gender is performed in society were different, but they would still choose to keep their assigned genders if swapping were on the table. Unfortunately, a lot of closeted trans people hear cis people complaining about the frustrating and problematic aspects of their gender and assume that everybody has the same low-grade dislike for their gender that they do.
Closeted trans people also assume that “I don’t hate being a man” is the same thing as “I enjoy being a man.” I can’t tell you how many of these questioning ladies tell me some variation of “I can’t be trans because I don’t hate being a man,” and then go on to describe countless little things they dislike about being seen as male, as if their gender were a pair of wet socks that they could never quite find a way to take off.
You might be surprised to hear that I didn’t actively hate being seen as a man before I came out to myself, either. Being seen as a guy wasn’t a constant source of misery for me. It just… was who I was, apparently, so I learned to just kind of live with it. A lot of people believe that you can only be trans if you feel actively hurt by being seen as a man, but that particular feeling won’t usually arrive until after you’ve started to transition and you finally know who you truly are. Before self-acceptance, your relationship with your assigned gender at birth is likely to feel a lot more like disconnection than distress.
I also can’t tell you how many times I’ve heard closeted trans women say something like, “well, I don’t hate being a man, and men have lots of institutional privilege. I don’t think I’d choose to be a woman, even if I could, because I wouldn’t want to give up my male privilege.” Male privilege is a real thing, of course, but it isn’t a reward that men get for having to endure the eternal discomfort of being men. Men enjoy being men, and they would still enjoy being men without their social privileges. If the only thing you like about masculinity is male privilege, that probably means something.
Consider That Gender Dysphoria Looks Different For Trans Women Who Haven’t Self-Accepted Yet
For years, I thought that I couldn’t be trans because I didn’t experience gender dysphoria. I was dead wrong.
One thing that kept me from realizing that I was experiencing dysphoria was the same reason that fish don’t know they’re swimming in water — it’s just what my life had always been like, so I thought being dysphoric all the time was normal human behavior. I knew that I was kind of sad and more than a little odd, and I knew that my experiences with masculinity were at least slightly gender non-conforming, but I was dealing with the pain of dysphoria every single day without having any idea what was actually going on. No matter how bad I felt, I could always come up with a good enough explanation that had nothing to do with gender.
The other problem is that gender dysphoria manifests differently in pre-acceptance trans women than it does in post-acceptance trans women. I always thought that gender dysphoria was the distress that you get from looking in the mirror and seeing a boy starting back at you instead of a girl, but that wasn’t a feeling I actually had until I started transitioning. You can’t get distressed about not seeing a girl in the mirror until after you’ve realized you’re a girl!
Before that, dysphoria manifests in dozens of other, much subtler ways. I wrote about my experience with pre-acceptance dysphoria here, in what has become my most popular essay ever. I highly recommend reading it in full if you are questioning your gender.
Consider The Null HypotheCis
In mathematics, a null hypothesis is something that is generally assumed to be true until it is proven false. It’s a default assumption, like “innocent until proven guilty.” If you’re going to convict someone of a murder, for example, circumstantial evidence just won’t do. You generally need overwhelming physical proof, or a confession, or some other obvious sign of guilt.
This excellent article by Natalie Reed argues that being cisgender (not trans) is treated as a null hypothesis by our society. We are all assumed to be our assigned gender at birth, and we feel as if we need overwhelming evidence to prove our transness. Otherwise, we continue to assume that we are cis.
This makes sense in the grand scheme of things, because there are probably more cis people in the world than trans people. As we discussed earlier, however, most people who are comfortable with their gender identity aren’t doing this kind of questioning. If you’ve arrived at this stage of self-discovery, there’s a fairly high chance that you aren’t completely cis.
The Null HypotheCis poses a simple and effective question: once you take your finger off the scale, how likely is it that you are trans? If you give the twin hypotheses of “I am cis” and “I am trans” equal weight, and you stop demanding that transness carry the full burden of proof, what feels right to you? If you start looking for proof of cis-ness the same way you look for proof of trans-ness, the whole illusion can sometimes come tumbling down.
Consider That If You Want To Be A Girl/Boy, Then You Are Already A Girl/Boy
It really is that simple. Men want to be men, and women want to be women. If you want to be a man, then you‘re a man. If you want to be a woman, then you’re a woman. If you don’t want to be either, or you want to be both, or you want to be a woman sometimes and a man other times, then you’re probably some flavor of genderfluid or non-binary.
“But you can’t just… do that!” I hear you say. But you absolutely can just do that. In fact, this is basically the one and only question you really have to answer for yourself. If you want to be a girl and you’ve always thought of yourself as a guy, then you will probably be happier living as a girl. It’s at least worth taking some steps to see if transitioning will bring you happiness, right?
Consider That Doubting Yourself Does Not Invalidate Your Possible Trans-ness
For years — decades, even — I “knew” that I wasn’t trans because “real” trans people are supposed to have an unshakable certainty in their own identity. I internalized this fictional image of a young trans woman demanding that everyone treat her like the woman she is, defiant in the face of oppression.
This is what being trans was like, I thought; bravery, courage, and absolute unwavering certainty in your identity. That wasn’t me, so I couldn’t be trans!
As it turns out, very few actual trans people feel this way before transition. Instead, we nearly all start out our journeys awash in self-doubt. That unwavering certainty does usually come, in time, but it can take months or years of self-acceptance as well as (in my case, at least) further validation in the form of hormone therapy and social transition.
But at the start, we nearly all feel like our gender is a confusing mess. We feel like we can’t possibly be trans enough to claim a queer identity, and we definitely don’t feel trans enough to transition. We worry that we are making the wrong decision, that we are overreacting, that stepping outside of our little cocoon of self-preservation is liable to be the biggest mistake we could ever make in our life.
If you feel all of this stuff, you’re in good company. My therapist even jokes that asking “am I trans enough?” is so common that it’s practically a symptom of being trans. You cannot figure out your gender identity without questioning it, and self-doubt is a normal part of that process.
Consider That Your Trans Journey Might Not Fit The Accepted, Popular Narrative
Popular culture has basically decided that there’s only one transfeminine story worth telling. It’s the story of a young trans girl who figures out her identity at a very young age. Even in childhood, she gravitates toward dolls and tea parties. She tries on her older sister’s dresses and begs her mom to buy her make-up and jewelry. She basically always looks like a girl, too — feminine facial features, short stature, thin and androgynous. If she doesn’t transition in childhood or adolescence, then she’ll still somehow make it to adulthood still looking more or less like a woman. She crossdresses all the time, and might even be a drag queen. She is also probably attracted to men, and might have worked a spell as a sex worker.
This is a valid and common trans narrative. I know many girls who have experienced some or all of these tropes. There’s a reason why this story is told over and over again, after all.
That said, the vast majority of trans women I know are nothing like this. Many of them had classically male childhoods, complete with toy cars, video games, and NERF guns. Many of them never cross-dressed at all, and felt somewhat repulsed by drag culture. Many of them grew up with large bodies, broad shoulders, and bushy beards. Many of them aren’t attracted to men at all, while others are bi or pansexual. Many of them did not begin seriously questioning their gender until their late twenties or early thirties. Many have no “signs” of being trans in their past. They simply spent their entire lives accepting that they were men, and that was that. Until it wasn’t.
This is a common trans narrative, but nobody really talks about it. Trans women like this — like me — have only really started to open up about our stories in the past few years. Before that? The only story you heard was the one I chronicled above. That’s why that trans narrative seems “right” and this one seems “wrong.”
But girls like us are incredibly common. This scientific study from 2003 (warning for dated language if you read it) chronicles the observations of a researcher who spent decades working with trans women. In her experience, there are three distinct groups of trans women, two of which follow the “I’ve always known” path I chronicled above, and one of which does not. According to her, “Group Three” trans women have classically male childhoods, tend not to show the normal signs of being trans, and tend to come out later in life. While some of them cross-dress, many do not, choosing to deal with their dysphoria in more subtle and internal ways. I can’t tell you how validated I felt reading that paper during my questioning phase, realizing that there were so many other trans women out there just like me.
I also believe that more trans women like us are coming out now because there’s so much more representation and so many more resources. In 1991, 2001, even 2011, the path to transition was much more difficult, and most people didn’t know any openly trans people. In this world, the only people who chose to transition were those for whom not doing so was just about impossible.
It isn’t just easier to question your gender here in 2021; it’s easier to gain access to trans communities, hormones, and other crucial resources. If I’d been born thirty years earlier, I might not have transitioned at all. If I’d been born thirty years later, I’d probably have transitioned as a teenager. Don’t worry about whether or not you’ve “always known” if this is the first time you’ve ever had the freedom and resources to truly ask yourself this question.
Consider That The Things Keeping You From Self-Acceptance Might Have Nothing To Do With Your Identity
Whenever I’m talking to a questioning trans woman, the conversation eventually turns to the obstacles that she might face if she chooses to transition. “I worry that I’m too tall/large/hairy/ugly to transition” is a pretty common fear. “I worry that my family will disown me/my partner will leave me” is another worry I hear a lot. Other girls are really worried about their career, education, or college situation. Many fear that they simply can’t handle the medical bills for HRT or trans surgeries.
Everyone — everyone — doubts that they have the fortitude to deal with socially transitioning. Coming out to friends, wearing women’s clothing, dealing with transphobia… it’s a terrifying mess, especially for closeted trans women, who usually feel pretty short on resilience as it is. The whole thing can seem chronically overwhelming.
These fears often manifest in the form of self-gatekeeping. “I’m afraid that I will never be a pretty girl” turns into “I can’t be trans, because what if I’m not pretty enough after I transition?” This seems somewhat silly in a vacuum, but pre-acceptance trans girls will sometimes do anything to convince themselves that they aren’t actually trans. I definitely thought that I wasn’t trans because I simply couldn’t imagine actually taking HRT and dressing like a woman every day. That was something that brave people did, not people like me, so I couldn’t be trans!
Why do we do this to ourselves? I think it’s all about self-protection. We know that transition is incredibly difficult, and so we will try literally everything else in the world before we’re even willing to start facing the “am I trans?” question. We develop really strong self-protective voices that push back hard against the truth because then we don’t have to worry about the terror of what comes next.
Here’s the thing, though: even if you are trans, you don’t actually have to do anything about it. While I highly recommend transitioning, it’s definitely possible to self-accept and then just… do nothing. Keep your name, your pronouns, your life as it is. Or you can just change a few things, and enjoy those little pings of gender euphoria where you can.
The important thing to remember is that the truth of your identity is separate from all of the hopes and fears you have about transitioning. If you’re a girl on the inside, it doesn’t matter what you look like. It doesn’t matter what your family thinks of you. It doesn’t matter whether or not you have the means or even the desire to medically transition. Identity is a mental and spiritual thing, separate from all of this. If you’re a girl, you’re a girl.
So start there. Figure out who you ARE, regardless of what you do about it.
Whenever I talk to a questioning trans woman who is stuck on this stuff, I always try to factor out these social factors as best I can. I’ll ask hypothetical questions like this:
You are given a magical button that will permanently swap your gender, giving you an “opposite-gendered” body that is equivalent to your own in age, fitness, and attractiveness. If you press the button, everybody in your life will have always known you as a girl. They will accept you immediately. You will not lose your partner, your job, or your family. Do you press it?
Cis people would not even consider pressing this button, by the way. If you know deep down that you’d press it but are still afraid to self-accept as trans, then your sticking point probably has more to do with your fear of transitioning than it does with your true identity.
Consider That It’s Rarely “Just A Fetish.”
I cannot tell you how many trans people — including me — began exploring their gender feelings in the realm of sexual fantasy.
There are many different ways for this to manifest: gender-play with partners, enjoying transformation-related drawings, reading stories about boys who are turned into girls, or role-playing gender transformation fantasies with partners on online forums or messaging apps. There’s so much of this stuff out there, and a lot of the people who enjoy it are closeted trans women like I was.
This makes a lot of sense when you think about it. Sex is one of the few realms of human experience where it’s safe to explore gender without having to face larger questions about identity. It’s extremely possible to separate these two things in your head for years and years and years. You’re just a man who occasionally likes to fantasize about being turned into a woman. That doesn’t mean you’re trans!
Unfortunately, exploring gender this way can actually make self-acceptance harder for many trans women. While I found this sort of sexual exploration absolutely necessary in my pre-self-acceptance days, it also meant that I was able to write off my intrusive gender thoughts or daydreams as “just a fetish.” I treated them as something hidden and shameful instead of something to investigate further.
This issue is further complicated by the term “autogynephilia,” a bogus transphobic “theory” posited by a crank psychologist named Ray Blanchard. Autogynephilia posits that many people who self-identify as trans women aren’t actually women at all, but are instead creepy men who are turned on by the idea of being a woman or having a vagina. According to Blanchard, their entire transition is just an elaborate fetish game that they’re forcing the world to participate in.
I want to be clear, here: autogynephilia is bullshit. It has been discredited by actual scientists and researchers many, many times. The entire point of this theory, as far as I can tell, was to try and get cis people to start viewing trans women as male sex predators. Thankfully, most cis people don’t feel this way, and most of them haven’t heard of Blanchard or autogynephilia at all.
Unfortunately, a lot of closeted trans women come across this stuff as they’re questioning and think, “oh, do I just have autogynephilia? Maybe I’m not actually trans.” This is doubly true for trans women who have spent a lot of time expressing their gender feelings in sexual spaces, especially if they feel sexually aroused by the idea of becoming a woman.
While this feeling of arousal is too complex to fully unpack in this tiny section of a much longer essay, I will say that this feeling is really common early on but it tends to fade as your transition progresses. Some of it has to do with the fact that if you tie gender euphoria to sexual arousal for long enough, one will express partially as the other. Some of it also has to do with the fact that being seen as your true gender, or experiencing sexual pleasure as your true gender, feels fucking terrific. Either way, it’s not “just a fetish” if your feelings go deeper than pure sexual arousal.
Consider The Broad Umbrella of Trans Identities
If you haven’t spent a lot of time in a community with openly queer people, you might not have fully internalized just how many different ways there are to both experience and express your gender.
The wider world makes it seem like the “man” box and the “woman” box are two entirely different things with a massive gulf of emptiness between them, but that’s not really true. There are a roughly infinite number of ways to express gender, both inside and outside those boxes, and your gender might be somewhere in that undefined space. I am a fairly binary trans woman, and I like being inside the girl box, but my conception of gender as well as how I choose to express it are often entirely different from other people who are also in the girl box.
There is no right way to be trans. Some trans people change their presentation but don’t change their pronouns. Some trans people change their name and pronouns but don’t change their presentation. Some trans people are okay living as their assigned gender at birth as long as they know who they are on the inside.
Many trans people don’t opt for gender affirming surgeries or hormones. Many trans people use a different name and different pronouns depending on how they’d like to be seen in a given situation. Many trans people simply forge a relationship to gender that is slightly askew from cisnormativity, plant their flag, and call it a day.
Many trans people set out to transition one way, and ultimately realize that their identity better matches with something that they couldn’t have even begun to see when their process started.
All of this is valid, and my goal by including all this stuff here is to take the pressure off. It’s harder to accept yourself as trans if you feel like self-acceptance is going to come with a whole new set of impossible expectations. In truth, one of the great joys of being trans is realizing that you are actually free from all of these narrow ideas about what gender can and cannot be.
No matter what you decide about your gender, the important thing is to be true to yourself. This sounds cheesy, but giving yourself permission to be honest about what does and does not bring you joy in terms of gender and gender presentation can be an explicitly radical act. This journey might lead you toward more comfort in your assigned gender at birth, or toward some sort of non-binary or gender-fluid identity, or perhaps you will come join me over here in the girl box (we have cupcakes!).
Whatever you choose, do it because it helps you feel more like yourself.
Consider That Transition Is Less About Discovering A Single Metaphysical Truth And More About Doing What Makes You Happy
One sticking point I come across a lot when I talk to questioning trans women is that they’ve paralyzed themselves with fear and are unwilling to act until they’ve solved the equation at the center of themselves and completely and fully accepted that they are, without a doubt, 100% trans.
Unfortunately, this is pretty much impossible to do, especially before you’ve taken any actions toward affirming your gender. There’s no blood test or brain scan that can confirm trans-ness, so you will never have unequivocal proof. I can’t tell you how many girls have messaged me weeks or months into their self-acceptance and said things like, “hey, so I actually had a good day today presenting as male. Does that mean that I’m not actually trans?”
(To answer: nope! I’ve had plenty of good days in boy-mode. I’m still a girl.)
To that end, it’s worth keeping in mind that you are not a puzzle to be solved. You do not have to perform an exact taxonomic classification of your own gender. You’re just a human with your own complex set of needs, desires, dreams, goals, fears, triggers, and a whole mess of everything else. You are a contradictory, complex, illogical being who contains vast multitudes.
This is kind of scary, but hopefully it’s also somewhat freeing. There’s no “proper” timeline to your transition. No list of things that you absolutely have to do. You can keep your name, or change it. You can get gender confirmation surgery, or you can keep what you’ve got. You can wear dresses every day, or you can leave them all for me. Some trans ladies have been dressing like women since they were old enough to buy clothes, but I didn’t once wear a full femme outfit until I was already three months into HRT. There are no rules. They were all made up by people who have been dead for hundreds of years.
You also don’t have to commit to anything right away. Transition isn’t one giant leap into the abyss — it’s a series of small, willing steps. All of the early steps are easily reversible, and you never have to do anything that you don’t think will help make your life better. If you keep your eyes on your feet, you’ll cross the chasm before you know it.
I like to recommend that people who are questioning their gender pick one or two small things and try them out instead of being stuck in their head all day, waiting for more evidence to present itself. Shave your arms, your legs, or your chest. Get some nail polish. Buy a piece of female clothing. Make an “alt” account on social media with a female name and she/her pronouns and engage with the digital world as a girl. Tell a trusted friend or two that you are questioning your gender, and ask them to call you by a different name/pronouns in private to see how it feels. Even the first few months of HRT are easily reversed, if you want to see how your mind works on estrogen.
While some of these steps are probably going to make you feel overwhelmed — heck, you might feel overwhelmed just thinking about them — you might also feel a few pings of absolute bliss somewhere in the process. Little moments of “oh, oh, OH, I like this, this feels good!!”
That’s gender euphoria, and it’s a sign that you’re proceeding in the right direction. If you follow those feelings, wherever they take you, I guarantee you it will lead to so much happiness and joy.
How is Gender Dysphoria Diagnosed?
This section is going to focus on the diagnostic criteria under the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders, version five (DSM-5). The reason I’m focusing on this standard is because, well, nobody else has one. The UK’s National Health Service basically mirrors the APA’s DSM. Other countries have their own local standards, but they’re all either very similar or a lot more outdated.
The WPATH SoC describes ways that gender dysphoria manifests, but does not define clear diagnostic criteria, instead leaving it up to individual mental health professionals to make their own diagnoses. In general, it advocates that, if the patient is of sound mind and body and says that they have gender dysphoria, they should be believed. The key piece here is “sound mind and body”; it is left to the mental health professional to do the due diligence to ensure that there are no other conditions which may be causing the patient to believe this.
Or, to put it bluntly, WPATH says that if you think you’re trans, you’re trans. This has been the attitude that the majority of the community has adopted as well. As long as you believe your gender does not match what you were assigned at birth, you are transgender. However, insurance companies aren’t so happy with self-diagnoses, so here are the criteria which are defined in the DSM-5 for diagnosing someone with gender dysphoria.
For Your Information
Diagnosis of gender dysphoria in prepubescent children requires the child must have a documented six month history of meeting six of these criteria (one of which must be Criterion 1), as well as demonstrated distress or impairment in social, school, or other important areas of functioning.
- A strong desire to be of the other gender or an insistence that one is the other gender (or some alternative gender different from one’s assigned gender).
- A strong preference for wearing clothes typical of the other gender.
- A strong preference for cross-gender roles in make-believe play or fantasy play.
- A strong preference for the toys, games, or activities stereotypically used or engaged in by the other gender.
- A strong preference for playmates of the other gender.
- A strong rejection of toys, games, and activities typical of one’s assigned gender.
- A strong dislike of one’s sexual anatomy.
- A strong desire for the physical sex characteristics that match one’s experienced gender.
Note These are the criteria for children. Adolescents and adults have a different set of criteria. Both sets can also be found here. I have also changed the wording slightly, here, as the official criteria are binary-centric.
For an adult to be diagnosed with gender dysphoria by a licensed mental health professional, they must meet two of these six criteria and have experienced those criteria for longer than six months.
-
A marked incongruence between one’s experienced/expressed gender and primary and/or secondary sex characteristics
The way the person sees the world and interacts with the world does not align with the way it is typically expected for someone of the gender they were assigned at birth. There are a very broad number of traits which fit into this description. It can be in the way they interact with others, how they talk, what hobbies they prefer, how they dress, their body language and mannerisms, what gender(s) they relate to more.
-
A strong desire to be rid of one’s primary and/or secondary sex characteristics
-
A strong desire for the primary and/or secondary sex characteristics of another gender
These two are pretty well paired. This is physical dysphoria as previously defined. The person finds discomfort with aspects of their body which are a result of their sex at birth.
-
A strong desire to be of another gender
-
A strong desire to be treated as another gender
These are the social and societal dysphoria. They are how a person wants to interact with the world, and wants the world to interact with them.
-
A strong conviction that one has the typical feelings and reactions of another gender
This is pretty self explanatory.
As I said, only two of these conditions need to be met for a formal diagnosis. You may notice that only two of these comprise the physical body. It is perfectly valid for a trans person to be experiencing gender dysphoria without actually hating any part of their body or wanting to change any part of their body. Physical dysphoria is only one fraction of the many things that lead to being trans.
Now, here is the kicker. If you identify as transgender, meaning that your gender does not align with the binary sex you were assigned at birth, you already meet two of these criteria! You have a strong enough desire to be of another gender that you are identifying that you are another gender, and you have a strong conviction of what your gender feels like, and it isn’t what you were given at birth.
So, it is literally impossible for a person to identify as trans and not experience gender dysphoria. By the WPATH requirements anyone can identify as trans. Ergo, the statement “you do not have to have dysphoria to be transgender” is a logical paradox.
Then why do we still say it? Because most people don’t know what gender dysphoria actually is, and it is easier to repeat the mantra than to explain the nuances and subtleties of how gender dysphoria manifests. But hey, look, now you’ve got a nice article to link to that can help people understand that.
How is Gender Dysphoria Treated?
Treatment options vary significantly depending on the individual person’s needs. Every single transition is unique, and there is no one way to transition. This section is a list of possible pathways.
Social Transition
In a phrase: coming out of the closet. This is simply announcing to the world that you are transgender. You announce that you wish to use a new name and/or new pronouns – or not; you may just wish for people to know that you are trans and do not actually identify with your assigned binary gender. For some non-binary people this may not even be a full step away from their assignment, since gender is a spectrum and there is such a thing as a “non-binary man” and a “non-binary woman”.
A social transition is the act of stepping out of the closet, and it can relieve a lot of stress from the suppression of oneself.
Legal Transition
This is the process of changing your legal documents to reflect your true gender. This may be through a legal name and gender change issued by a court, through a change of gender marker on an official ID, or through re-issuing of birth certificates and marriage licenses.
Presentational Transition
These are changes to how you style yourself, be it your clothes, your hair, or the use of makeup. Our society heavily genders all of these things, and switching presentation is both affirming to one’s self and also sends cues to those around them about how they wish to be addressed.
Medical Transition
For adults, this is hormone replacement therapy and surgery. For adolescents, this often means puberty blockers until the teen is old enough to be certain of which gonadal hormone they want to have. For prepubescents, this is nothing. Let me repeat that again, since transphobes keep getting it wrong.
PREPUBESCENT CHILDREN DO NOT MEDICALLY TRANSITION.
While the American Academy of Pediatrics strongly encourages the validation and acceptance of transgender youth, and the enabling of all other forms of transition, they explicitly do not support doctors beginning either hormone therapy or puberty blockers until a child has reached Tanner stage 2.
Furthermore, no surgeon in the United States will perform a gender altering surgery on a minor (excluding intersex “corrections”, which is a whole other problem outside the scope of this article). Very few children have strong enough features to be read as either male or female without clues provided through presentation. Allowing a child to change their hair and clothes is all that is needed for the child to be seen as male or female.
Hormonal Transition
Masculinizing hormone therapy (female to male sexual characteristics) consists of the introduction of testosterone, usually via intramuscular injection or topical gel. The increase in total gonadal hormones typically causes a cessation of ovulation, which is the source of the majority of estrogen produced in the ovaries.
Feminizing hormone therapy (male to female sexual characteristics) consists of the introduction of estrogen, typically estradiol, via oral pills, patches, or regular injections (intramuscular or subcutaneous). The use of slow dispensing implants is also becoming more and more common. It is also common practice to prescribe an anti-androgen to block testosterone production or absorption. In the United States this is usually spironolactone, a blood pressure medication which has a testosterone blocking side-effect. Outside of the US, the most common drug is cyproterone acetate, an androgen receptor blocker, which is not available in the US. Doctors may also prescribe bicalutamide, which also blocks androgen receptors. However, some doctors may simply opt to use larger estradiol doses in order to cause the body to halt testosterone production.
In adolescents, puberty blockers may involve the above androgen blockers, or (if it is covered by insurance) the use of an antigonadotropic (a drug which blocks the hormones that cause the production of estrogen and androgen) such as leuprolide acetate (a shot delivered every few months) or histrelin acetate (an annual implant).
Surgical Transition
Transgender surgeries are typically divided into three separate categories:
Bottom Surgery (modifications to genitals):
-
Feminizing:
- Orchiectomy (removal of the testicles)
- Scrotectomy (removal of scrotal tissue, following orchiectomy)
- Vasectomy (removal of the sperm ducts, which is done during orchiectomy but can also be done before on its own)
- Vaginoplasty (creation of a vaginal cavity)
- Vulvoplasty (creation of a vulva, with or without depth).
For Your Information
A newly developing area of bottom surgery is in AMAB non-binary operations which attempt to perform vaginoplasty without the removal of the penis. This particular surgery is extremely experimental and has been performed less than a dozen times in the United States, but the outlook for the future is good.
An additional option for non-binary bottom surgery is genital nullification surgery, which aims to completely remove the external genitalia, leaving only a urethral opening.
-
Masculinizing:
- Hysterectomy (removal of uterus and cervix)
- Oophorectomy (removal of one or both ovaries)
- Salpingectomy (removal of one or both uterine tubes, often performed with hysterectomy and/or oophorectomy)
- Vaginectomy (removal of vaginal cavity)
- Metoidioplasty (a process which turns the enlarged clitoris after hormone therapy into a penis)
- Phalloplasty (construction of a penis from skin grafting)
- Urethroplasty (extension of the urethral canal through the phallus)
- Scrotoplasty (use of labia majora and prosthetic testicles to construct a scrotum).
Phalloplasty does not necessarily require previous hormone therapy. While it is common to perform vaginectomy, urethroplasty, and phalloplasty at the same time, urethroplasty and vaginectomy are not technically required to construct a penis. However, as vaginal tissue is typically used to construct the new urethra, some surgeons will not perform urethroplasty without vaginectomy.
Top Surgery (modifications to the chest)
-
Feminizing:
- Breast augmentation via fat transfer or implants.
-
Masculinizing:
- Bilateral mastectomy (breast tissue removal) with chest reconstruction
- Breast reduction (some fat and breast tissue removal)
Mastectomy for top surgery typically reshapes the nipples to be more masculine, but some people opt to remove their nipples entirely.
Facial Feminization / Masculinization Surgery (modifications to the skull, cartilage, and skin on the face).
The younger a person is, the less they will need these surgeries, especially if they medically transition prior to the age of 20.
-
Feminizing:
- Forehead recontouring
- Eye socket recontouring
- Brow lift
- Hairline correction
- Blepharoplasty (lifting of eye bags)
- Rhinoplasty (reshaping of the nose)
- Cheek implants
- Lip lift
- Lip filling
- Jaw recontouring
- Tracheal shave (adam’s apple reduction)
- Rhytidectomy (face lift)
-
Masculinizing:
- Forehead augmentation
- Jaw augmentation
- Chin augmentation
- Tracheal augmentation (adam’s apple enlargement)
Other Trans Feminine Surgeries:
- Brazilian Butt Lift: Fat from the belly is transplanted into the butt in order to increase hip to waist ratio.
- Voice Feminization Surgery: An incision is performed in the vocal cords in order to permanently raise the pitch.
- Cinderella Surgery: Bones in the foot are shortened in order to reduce foot size. EXTREMELY RISKY
- Shoulder Reduction: The collar bone is shortened to reduce the width of the shoulders. EXTREMELY RISKY
What is the Cause of Gender Incongruence?
To put it bluntly, we don’t know (at least not firmly). Science and modern psychology has proven that it is not caused by nurture; no one becomes transgender, gender identity is congenital, solidifying before we even exit the womb. It also appears to sometimes be hereditary; transgender parents have a higher likelihood of having transgender children, and many times they realize this in reverse. The child comes out to the parent, and that helps the parent realize they can come out as well.
Here is the science that is believed to influence gender identity. This does not mean that it defines gender identity, nor does it fully encapsulate one’s gender, as so many aspects of gender are cultural and social. None of this is prescriptive of a person’s identity, none of it is cast in stone.
If you’ve seen Jurassic Park, you may remember this scene:
 This isn't science fiction, although it is very simplified.
This isn't science fiction, although it is very simplified. 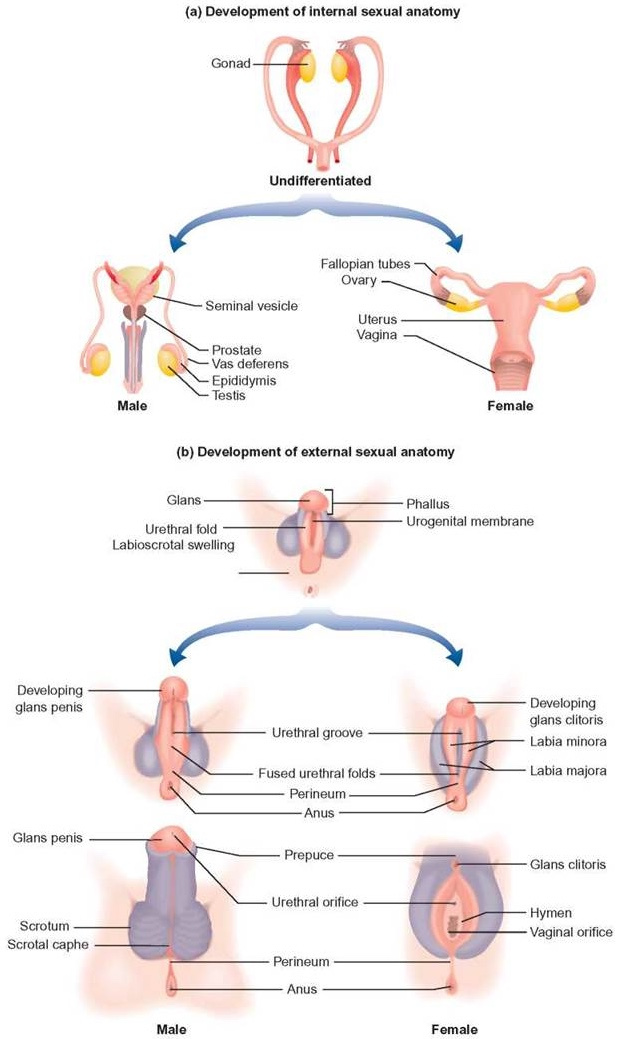
The gonads in human fetuses initially develop in a bi-potential state, meaning they can become either ovaries or testes. The SRY gene on the Y chromosome releases a protein called testis-determining factor (TDF). This protein then starts a chain reaction with SOX9 production (another protein), which causes the gonadal cells to form into the Sertoli and Leydig cells that make up the testes. If TDF is never produced or is interfered with, the gonad cells form into the Theca cells and follicles which comprise the ovaries.
Once formed, the testes then begin producing a testosterone surge which typically starts in the eighth week of gestation and continues until the 24th week. This surge, combined with another hormone from the placenta, is responsible for the development of the penis and scrotum. Genitalia formation starts around week nine and becomes identifiable by the 11th week. If the surge does not occur, or the body does not respond to it (such as in the case of androgen insensitivity syndrome) then the genitalia form into the vulva, vagina, and uterus instead.
If there is an interference in this process then you can end up with the wrong bits, and this is the result of many intersex conditions. Oftentimes this is a partial development, where the external genitalia only partially form but functional gonads still exist. Sometimes the child comes out with fully functional male or female genitalia, but mismatched gonads. Sometimes the TDF protein fails to release and the fetus grows completely functional female reproductive organs, despite the presence of a Y chromosome.
This is known as Swyer syndrome, and an unknown number of women may have this condition. In 2015 an XY woman with Swyer syndrome who was born without ovaries successfully carried and gave birth to a child via IVF. Usually, Swyer syndrome results in completely non-functional ovaries, but in 2008 a woman was found with Swyer syndrome who had gone through puberty, menstruated normally, and had two unassisted pregnancies. Her condition went undiscovered until her daughter was found to also have it.
The fact is, the vast majority of the population has never been tested for genetic karyotype, so we don’t know how common these cases actually are. Where does this come into effect for gender identity? Well, the exact same process that causes the external genitals to differentiate also occurs for the brain.
 Lisa T Mullin
Lisa T Mullin Brain Split
The prenatal brain doesn’t really start to develop until between week 12 and 24. The cerebral cortex, the thin outer layer of the brain that contains most of what we think of as consciousness, grows substantially during those periods of time. Prior to that, the structure present is more like a scaffolding — the basic parts of the nervous system necessary for bodily function. The primary sulci (the wrinkles in the cerebral cortex that allow for more surface area) start to form at week 14, well after the genitals have developed.
It has been confirmed multiple times via MRI studies that there are small but significant differences between cis male and cis female brains — differences which align with the gender identities of trans people in the study. Note that this does not mean that anyone with those differences will have that gender; gender identity isn’t that simple, but it provides evidence that there is a clear difference in masculine and feminine brains. There is also evidence that brains can have mosaic combinations of these differences, which may be the case in non-binary people.
A change in the testosterone levels in the fetus after the 11th week can directly impact the masculinization of the cerebral cortex, as well as changes in other parts of the brain structure. This has been examined over and over again in studies of female-assigned children with CAH (congenital adrenal hyperplasia) and CAIS (complete androgen insensitivity syndrome).
We found a significant relationship between fetal testosterone and sexually differentiated play behavior in both girls and boys.
— Fetal Testosterone Predicts Sexually Differentiated Childhood Behavior in Girls and in Boys
An excess of testosterone in the mother’s body during the second trimester can (and does) cause masculinization of the brain in an externally female fetus, and an interference in testosterone production or uptake can (and does) cause feminization of the brain in an externally male fetus. This interference does not have to be external in origin, either. Any number of genetic traits can cause the brain to respond differently to testosterone.
A fairly large study of transgender individuals released in 2018 found several key genes which were statistically more likely to be longer among trans women (longer as in having more repeated fragments). Individually these genes may not have an impact strong enough to cause a malfunction of masculinization, but collectively they absolutely could reduce the ability for the fetal brain to masculinize. These genes are all passed from parent to child, giving credence to a tendency for trans parents to have trans children.
Gender is Biological
Sadly, western society has actively prevented a deeper understanding of gender. Ancient civilizations understood it well, but colonialism wiped them off the map. 100 years ago, scientists in Germany were actively studying transgender medicine and made extraordinary advancements, until the Nazis burned it all in 1933. Conservative and fascist pressures in the modern day have hindered advancements in transgender healthcare whenever possible.
Yet, progress continues, and every few years we learn a little bit more.
What we know for certain is that it is not a psychological condition. It is not something caused by trauma or by any external influence; nothing can make a person transgender. It happens in the womb, and is not something that a person can choose to be, any more than they could choose their race or their eye color. It has nothing to do with sexual orientation, it has nothing to do with kinks or fetishes, and it has nothing to do with social influences from their parents or from their peers. Transgender children are as firm in their identities as cisgender children are.
But the Chromosomes!!!
More than Two Options
TransEthics™ #BlackTransLivesMatter @TransEthics
#BlackTransLivesMatter @TransEthics I'm going to regret paying the co-pay for this test eventually because it was pretty pricey… but I had my karyotype done. Just got the results.
I –a trans woman– have XX chromosomes.
the GC crowd can g[REDACTED]k themselves
There are dozens of ways that chromosomes can be much more complex than XX and XY. Referred to as DSDs (differences in sex development), not all of them result in an intersex condition, and many only manifest at the onset of puberty.
-
De la Chapelle syndrome (46,XX Male) occurs when the SRY gene from the sperm parent crosses over into a non-Y-bearing sperm during spermatogenesis. When the egg and sperm merge, it results in an XX embryo with an SRY gene, creating a phenotypically-male child with two X chromosomes.
-
Swyer syndrome (46,XY Female) produces a phenotypically-female child with an XY chromosome. This results from a dozen different genetic conditions, including:
-
XX gonadal dysgenesis is very similar to Swyer syndrome, except it occurs in XX children and results in nonfunctional ovaries.
-
Turner syndrome (45,X) produces a phenotypically-female child with numerous abnormalities. It occurs when neither an X or Y chromosome crosses over from the sperm.
-
Klinefelter syndrome (47,XXY) results in a phenotypically-male child with more feminine traits. In extremely rare cases it appears in female-assigned children as well, resulting in feminized testicles instead of ovaries.
-
48,XXXY Klinefelter syndrome has similar results to 47,XXY Klinefelter syndrome, but with more intense health issues.
-
49,XXXXY Klinefelter syndrome is often fatal, but when it isn’t, it often results in a sterile child.
-
Trisomy X (47,XXX), Tetrasomy X (48,XXXX), and Pentasomy X (49,XXXXX) all result in a female child, but with progressively more intense health issues.
-
XXYY Syndrome results in male children (due to two SRY genes) who often experience hypogonadism, needing testosterone supplements, but otherwise seeming like a typical male.
-
Mosaicism results when some cells in the body have one set of chromosomes and other cells have another due to a mutation of the genome during gestation. This may be XX/XY (resulting in a dual set of genitalia), X/XY (a milder form of Swyer or Turner syndromes) or XX/XXY (a milder form of Klinefelter syndrome).
-
Chimerism occurs when two fertilized embryos merge together into one zygote, causing half of the child to contain one set of DNA and the other half to contain another. This can result in an otherwise completely typical human being of either male or female phenotype, even capable of producing offspring, but which comes back on a karyotype test as not matching their phenotype based on where the sample was taken on their body. In extremely rare cases this can result in two full sets of reproductive organs.
-
Congenital adrenal hyperplasia (CAH) is masculinization of the female genitals in an XX child due to overactive adrenal glands.
-
Androgen insensitivity syndrome (AIS) is a total or partial resistance to all androgens, preventing masculinization of all organs, save for the testicles, in an XY child. AIS subjects typically develop a female gender identity, but some partial cases may be male.
-
5-alpha-reductase deficiency (5ARD) is a failure in the body’s ability to metabolize testosterone into dihydrotestosterone (DHT), preventing masculinization of the genitalia until the onset of puberty, when the child suddenly grows a penis.
-
Aromatase deficiency causes masculinization of an otherwise female child due to excess levels of testosterone (and can bleed over into the mother during gestation).
-
Aromatase excess causes feminisation in an otherwise male child, as all testosterone is converted into estrogen.
 Open Ocean Exploration @RebeccaRHelm
Open Ocean Exploration @RebeccaRHelm Friendly neighborhood biologist here. I see a lot of people are talking about biological sexes and gender right now. Lots of folks make biological sex sex seem really simple. Well, since it’s so simple, let’s find the biological roots, shall we? Let’s talk about sex...[a thread]
Open Ocean Exploration @RebeccaRHelm If you know a bit about biology you will probably say that biological sex is caused by chromosomes, XX and you’re female, XY and you’re male. This is “chromosomal sex” but is it “biological sex”? Well...
Open Ocean Exploration @RebeccaRHelm Turns out there is only ONE GENE on the Y chromosome that really matters to sex. It’s called the SRY gene. During human embryonic development the SRY protein turns on male-associated genes. Having an SRY gene makes you “genetically male”. But is this “biological sex”?
Open Ocean Exploration @RebeccaRHelm Sometimes that SRY gene pops off the Y chromosome and over to an X chromosome. Surprise! So now you’ve got an X with an SRY and a Y without an SRY. What does this mean?
Open Ocean Exploration @RebeccaRHelm A Y with no SRY means physically you’re female, chromosomally you’re male (XY) and genetically you’re female (no SRY). An X with an SRY means you’re physically male, chromsomally female (XX) and genetically male (SRY). But biological sex is simple! There must be another answer...
Open Ocean Exploration @RebeccaRHelm Sex-related genes ultimately turn on hormones in specifics areas on the body, and reception of those hormones by cells throughout the body. Is this the root of “biological sex”??
Open Ocean Exploration @RebeccaRHelm What does this all mean?
Open Ocean Exploration @RebeccaRHelm It means you may be genetically male or female, chromosomally male or female, hormonally male/female/non-binary, with cells that may or may not hear the male/female/non-binary call, and all this leading to a body that can be male/non-binary/female.
Open Ocean Exploration @RebeccaRHelm Biological sex is complicated. Before you discriminate against someone on the basis of “biological sex” & identity, ask yourself: have you seen YOUR chromosomes? Do you know the genes of the people you love? The hormones of the people you work with? The state of their cells?
Open Ocean Exploration @RebeccaRHelm Of course you could try appealing to the numbers. “Most people are either male or female” you say. Except that as a biologist professor I will tell you...
Open Ocean Exploration @RebeccaRHelm The reason I don’t have my students look at their own chromosome in class is because people could learn that their chromosomal sex doesn’t match their physical sex, and learning that in the middle of a 10-point assignment is JUST NOT THE TIME.
 plant lesbian @alicemiriel
plant lesbian @alicemiriel @RebeccaRHelm As a fellow genetics lab teacher, this is the same reason my department stopped chromosome testing in lab. A really cool experiment would turn into guys getting freaked out they have XXY, etc.
But Most People Are Still XX or XY!!!
Biological sex in endosex (non-intersex) people is still more complicated than the simplistic XX/XY model suggests. Even if someone has typical 46,XX or 46,XY chromosomes, the body can change how it uses DNA without changing the DNA sequence itself. This process is called epigenetics.
Epigenetic changes vary between XX and XY chromosomes, but they also differ as people age in sex-specific ways. Long-term gender-affirming hormone therapy appears to make some of those sex-and-age-specific changes more masculine on testosterone, or more feminine on estrogen. Therefore, the DNA of a cis man isn’t used the same way as the DNA of a trans woman on estrogen, even if they both have XY chromosomes, and the DNA of a cis woman isn’t used the same way as the DNA of a trans man on testosterone, even if they both have XX chromosomes.
How Hormones Work
As we described in the Causes of Gender Dysphoria section, every human’s DNA contains the genetic instructions for both male and female bodies, and which set of instructions gets used is controlled by what hormones your gonads produce. That differentiation occurs entirely based on whether you happen to have an SRY gene which, between the sixth and eighth weeks of gestation, kicks off a chain reaction that produces testes instead of ovaries. From that point on, every sexual attribute of the human body (primary and secondary) is a result of the hormones that those gonads produce.
If they produce estrogens (primarily estradiol), the genitals form into a vulva, vagina, and uterus. If they produce androgens (primarily testosterone), the genitals form into a penis and scrotum, shifting the Skene’s gland downward and enlarging it into a prostate. Differentiation ends here until the onset of puberty, nine to ten years later, and we all know what puberty does.
So how does this work? Why do the cells differentiate like this? Well, before we can explain that, first we have to explain the concept of a receptor.
Hormone Receptors
In simplest terms, a receptor is like the keyed lock ignition on a car (do new cars still have keyed ignitions?). Every cell in the body has a set of locks which activate different functions within that cell. They’re like switches which signal to the cell that it should activate a different part of its genetic sequence. Each receptor can only accept certain chemical compounds, much like how a lock can only accept certain keys, and different chemicals have different capabilities at turning the key. Some can completely start the car, while others only turn it to Accessory Mode.
The ability for a chemical to fit into a receptor is called relational binding affinity, and is measured as a percentage of how likely a chemical will bind to a receptor compared to another. So, for example, if hormone B binds only 10% of the time in relation to hormone A, then it is said to have a 10% binding affinity. Similarly, the ability for a chemical to turn the key is called transactivational ability. Compounds which fit into a receptor but don’t do anything are called antagonists; compounds which are able to turn the key are called agonists. If it can only turn the key a tiny bit, it’s called a partial agonist.
You can think of antagonists like bouncers at a club. They stand in the doorway and prevent anything else from getting through, but don’t enter the club themselves. Most antagonists are referred to as blockers. This is different from an inhibitor, which is a compound that slows down a chemical reaction, or an activator, which speeds up a reaction. In receptors, an inhibitor lowers the ability of the receptor, causing it to respond less effectively to things that bind to the receptor, and an activator increases the ability of the receptor, making it respond stronger, like a booster.
In some cases, a hormone can function as an inhibitor or an activator for a different hormone by slowing down or increasing behavior in a cell. For example, progesterone increases cell activity, making cells respond more effectively to estrogens and androgens, and testosterone increases the transactivational ability of dopamine receptors, so less dopamine is needed in the brain for the same effect.
What’s in a Hormone
There are four main kinds of hormones:
- Amino acids such as melatonin (which controls sleep) or thyroxine (which regulates metabolism).
- Peptides like oxytocin and insulin, which are collections of amino acids.
- Eicosanoids that are formed from lipids and fatty acids and predominantly affect the immune system.
- Steroids, which signaling molecules produced by various internal organs in order to pass messages to other organs within the body.
 All steroids are formed from cholesterols (top left) and are derived from other steroids. Progestogens form into androgens which form into estrogens. This is a one-way exchange, and does not reverse, so don't believe it when someone tells you that too much estrogen will turn it into testosterone.
All steroids are formed from cholesterols (top left) and are derived from other steroids. Progestogens form into androgens which form into estrogens. This is a one-way exchange, and does not reverse, so don't believe it when someone tells you that too much estrogen will turn it into testosterone. For the purposes of transition, this last category is what we care about the most, as all of the sex hormones are steroids. They fall into seven main categories:
The first three of these are what we care about most when it comes to hormone therapy. Note: All human beings, regardless of phenotype, have some of every one of these hormones in their bodies. The ratios are what affect body shape.
Androgens
There are nearly a dozen different androgens, but the ones we care about the most are testosterone and dihydrotestosterone.
Testosterone is the primary masculinizing hormone for the human body and is produced in the adrenal glands, the testes, and in the ovaries (where it is immediately converted into estrone and estradiol). It tells both muscle and bone cells to grow and, in higher concentrations, encourages larger muscle mass and thicker skeletal structure. This also means that testosterone is critical for bone health, as it affects calcium distribution within the skeletal structure. Thus, severe depletion of testosterone can result in osteoporosis and fragile bones. Testosterone also plays a major role in sex drive and libido, encouraging mating behavior within the cerebral cortex.
Dihydrotestosterone (DHT), which is converted from testosterone in the prostate, skin, and liver, plays a major role in the development of the male genitalia during puberty by inducing random erections, and the growth of facial and body hair. Paradoxically, DHT is also what causes male pattern baldness, as it chokes off blood circulation to the follicles on the top of the scalp (sorry, trans guys, it’s a double-edged sword). DHT binds to androgen receptors ten times more strongly than testosterone, which is why it is critical to eliminate it for feminizing transition.
Estrogens
There are four estrogens: estradiol, estrone, estriol and estetrol. The latter two are only produced during pregnancy and are important for fetal health, but have no bearing on transition.
Estradiol is the feminizing hormone, as it is the primary signaling hormone for growth in the mammary glands (breast tissue), and because it encourages fat deposits in the thighs, hips, butt, chest, and arms, while discouraging fat deposits in the abdomen, thus producing a curvier figure. Estradiol also promotes increased collagen production, resulting in softer skin and more flexible tendons & ligaments.
Estrone’s role in the body has been something of a puzzle in medical research, as it has significantly lower binding affinity compared to estradiol (0.6%) and very low transactivational ability (4%). The hormone doesn’t appear to do anything; it just sits in the bloodstream. However, it has a unique ability to convert to and from estradiol via an enzyme group called 17β-HSD, making it ideally suited to function like an estrogen battery within the body.
New research is starting to suggest that the body may regulate total estradiol levels by releasing HSD17B1 to turn estradiol into estrone, and releasing HSD17B2 to convert it back, but this is a very early study. Both enzymes are produced in breast tissue, and may play a role in the presence of cyclical period-like symptoms in estrogenic individuals who do not have ovaries, such as trans women.
For Your Information
Why aren’t AFAB trans people prescribed estrogen blockers alongside testosterone?
There are two separate sources for estrogens within the female reproductive system. Ovaries contain thousands of follicles: cell structures which produce eggs. The pituitary gland produces luteinizing hormone (LH) and follicle-stimulating hormone (FSH), which encourages the follicles to grow into luteal cells. Theca cells within the follicle produce testosterone, and granulosa cells produce the enzyme aromatase, which converts that testosterone into estradiol. This is the first source of estrogen, but it is not the largest source.
Note: This is why PCOS causes ovaries to produce testosterone; the ovarian cysts disrupt the aromatase production, so the testosterone does not get converted.
Two weeks into the period cycle the hypothalamus tells the pituitary gland to produce an LH and FSH spike three to four times stronger than earlier in the cycle. That surge causes the follicles to swell until one pops, releasing an egg, at which point the remains of the follicle become a structure known as the corpus luteum. That corpus luteum then begins to produce progesterone and significantly more estrogens in order to prepare the womb for a fertilized egg. This is the second source.
Taking testosterone causes the hypothalamus to deactivate the genes that initiate this LH and FSH spike, so the follicles never reach maturity, ovulation never occurs, and the corpus luteum is never formed, removing a significant source of estrogen within the ovaries.
So no, Reddit, it isn’t just “because testosterone is stronger”, it’s because ovaries are a hell of a lot more complex than testes and are easier to disrupt. Please stop spreading this falsehood.
Progestogens
The primary progestogen is progesterone, which plays numerous roles in the body and has been found to be an important component for feminizing hormone therapy.
One of the largest roles that the progestogen receptor plays is in the regulation of gonadal function (ovaries and testes). The hypothalamus is positively littered with progestogen receptors and responds strongly to their activation, downregulating the production of GnRH, which then reduces the production of luteinizing hormone by the pituitary gland.
LH is what tells the ovaries and testes to produce estrogen and androgens. LH and its sibling hormone FSH both play central roles in ovulation, which is another large source of estrogen in ovary-havers. Thus, synthetic progestogens (chemicals that fit into progestogen receptors) are often included in birth control in order to prevent ovulation. In AMABs, progestogens are a useful tool for blocking testosterone production.
Another type of cell that is full of progestogen receptors is mammary tissue. Progesterone plays a major role in the growth and maturation of milk ducts within breast tissue. While little formal research has been conducted into progesterone’s effect on breast development, anecdotally it has been seen widely across the transfem community to provide significant improvements in breast fullness. Progesterone has also been demonstrated to increase blood flow to breast tissue, and encourages fat deposits in the breasts, both of which increase breast size.
Additionally, progesterone promotes better sleep, improves cardiovascular health, increases ketogenesis (reducing triglycerides), increases metabolic function, and has been found to reduce breast cancer risk.
Mineralocorticoids
Mineralocorticoids play no role in transition, but they are worth mentioning because of one major hormone: aldosterone.
Aldosterone is what instructs the kidneys to stop extracting water from the bloodstream. It is produced by the adrenal glands in order to regulate body hydration. Why is this significant?
Because one drug that is very commonly used in trans hormone therapy is an extremely powerful aldosterone antagonist: spironolactone. Spiro binds to mineralocorticoid receptors more strongly than aldosterone does, but does not activate the receptor. It just clogs it, preventing the kidneys from receiving the signal to stop extracting water.
This is why spiro makes people pee so much.
Androgenic Second Puberty 101
What To Expect from Masculinizing HRT
This is a compilation of reported medical transition changes collected from testimonials of AFAB trans people taking testosterone hormone therapy. This information is gathered from social media and chat rooms. Yes, that means this is all anecdotal, but historically, most of transgender medical study is anecdotal because no one wants to fund transgender medical research.
Note that this is a list of possible changes. There is no guarantee that every person on masculinizing HRT will experience all of these. Your age, genetics, medical history, degree of feminization from natal puberty, and hormone regimen can all have impacts on results. There is also just a degree of randomness — every body is different — and some things can take years to appear.
Voice Drop
Androgens cause the tissue that comprises the vocal cords to thicken and harden, permanently lowering the pitch of the voice. This is not a very fast change, but rather incremental over the first few years. Some people do not experience any voice change at all, it varies person to person. The change will not be drastic; if you are a soprano, you are not going to become a bass, but it could bring you down to a contralto or tenor.
This does not mean that your voice will automatically become read as male. Pitch is only a piece of how people gender voice, and the way you speak plays a much larger role. Vocal training will be needed to amplify resonance and change speaking style.
Changes in Body Temperature Placement
 Adam, the ever curious mf'er
Adam, the ever curious mf'er Androgens encourage extra blood flow to the extremities, making them warmer. Because of this, men have cooler cores but warmer oral and surface level temperatures. You may see your basal body temperature increase. The net result is that you will feel warmer, and likely will not be able to layer clothing as much as previously possible. If you live in cold climates, exposing your calves can help to dissipate heat without chilling you too severely.
This change often comes fairly early on; expect night sweats while your system gets used to it.
Changes in Perspiration
With the above shift in temperature distribution, this also results in a significant change in how one sweats. Sweat will pool on the head, back and armpits. You’ll also likely sweat more often, so keep water handy.
Body Odor
Often one of the first things to change: sweat and general body odor will become much stronger, especially during exercise. The smell will take on a sour, muskier smell. Tends to even out over time.
Body Hair, Everywhere
Androgens significantly increase the presence of body hair on the legs, groin, buttocks, chest, back, and arms. Hair will grow in thicker, longer, and darker. This will likely happen well before facial hair growth, which can take over a year to start. Rogaine/minoxidil can help with that, but be careful, as it is poisonous if ingested (especially to cats).
Male Pattern Baldness
MPB is caused by dihydrotestosterone (DHT), an androgen which metabolizes from Testosterone. Having more T in your body means more DHT can form, and the gene that contributes to MPB causes the hair follicles on the scalp to receive less blood, choking them out until the follicles die. There will likely be some loss of hair line eventually, no matter what, but if there is a history of baldness among the men in your family, then you can expect to see that as well. Again, minoxidil can help with this.
The synthetic androgen nandrolone does not metabolize into DHT and may be a viable alternative in place of direct testosterone if hair loss is a concern. However, DHT is important for genital growth, so this is a double-edged sword.
Thicker and Oilier Skin
Testosterone promotes the thickening and toughening of the epidermis, causing skin to become coarser. As estrogen levels fall, the body will produce less collagen. This causes the skin to become tougher and drier (especially in the knees and elbows). Veins on the hands, arms, and legs may become more pronounced, but not varicose.
Expect your face and scalp to become oilier. Acne is likely to be a problem, and not just on the face. This tends to be worst immediately after dosing. This will generally improve after the first few years.
Larger Hands / Feet
Over long periods of time (3-5 years) the hands may become tougher and more calloused. You may need to increase your ring size eventually.
Testosterone also causes ligaments and tendons to retain more water, altering their flexibility. Over time this can result in an increase in foot size as the arch of the foot lowers.
Thicker and Stronger Nails
Both fingernails and toenails will grow thicker over time as keratin levels rise due to the presence of androgens.
Increased Muscle Mass
Androgens stimulate muscle growth, which is why anabolic steroids (which are literally testosterone) are so common amongst bodybuilders. The body will naturally gain more muscle without even having to exercise, but with exercise there can be substantial gains, particularly in the arms and shoulders. Beware; you won’t know your own strength at first.
Added lean muscle in the upper body redefines the shoulder and neck line, creating a more masculine silhouette. It also improves the body’s ability to process lipids, making weight loss easier.
Fat Redistribution
Where estrogen encourages the body to deposit fats into the thighs, buttocks, and hips, androgens encourage the body to deposit fats largely into the abdomen. Starting testosterone will encourage your body to follow the androgen pattern, so you can expect new weight to deposit into your belly, while weight loss will take away from all over. Fat in the breasts, thighs and buttocks will slowly shift away as muscle builds, but this may take a long time.
Facial Feature Changes
Along with body fat migration, fat in the face also moves. The neck, chin and jawline will fill out while the lips and upper cheeks shrink. The color of the eyes may also change and become fainter in the long term, as testosterone causes the pigmentation in the iris to fade.
This is an extremely subtle and slow moving process that takes years, and it is easy to think nothing is changing at all. The greatest shifts seem to happen in years 3 and 4. Take selfies to compare.
Increased Tolerance of Caffeine, Alcohol, and/or Psychotropics
More mass means more blood to dilute chemicals into. Increasing testosterone also means a higher metabolic rate, increasing the speed at which toxins are removed from the bloodstream.
Mental Changes
As covered in the Biochemical Dysphoria section, brains can be wired for a certain hormone profile, and running on the wrong profile is like using a laptop with low batteries or an overheated processor. Starting HRT almost universally results in a cessation of depersonalization and derealization (DPDR) symptoms within the first two weeks. A mental fog lifts, and it becomes easier to concentrate on complex concepts (assuming you don’t also have other mental processing difficulties such as ADHD).
ADHD
If you have ADHD, there may be some changes in your symptoms. Androgens amplify dopamine receptor function, so increasing testosterone can improve the activation potential for dopamine in the brain. Dopamine is a key neurotransmitter in the behavior of working memory, the short-term memory of the brain. More working memory means you may become less prone to distractions and have an easier time maintaining cognitive load.
However, estradiol encourages the production of dopamine, so as estrogen levels fall there will be less dopamine for the brain to work with. Your symptoms worsen, not improve.
Emotional Expansion
The alleviation of DPDR almost universally is accompanied with a much broader capacity for emotion and emotional regulation. Emotions become somewhat more controllable and suppressible, less likely to overwhelm on the spot. Please note: suppressing emotions is a very quick way to develop trauma.
However, the ability to express them may become reduced. Some people lose the ability to cry after starting on testosterone, but this is not a universal experience and may be tied into how strong your T dose is. The reasons behind this aren’t well known, although some studies have found that androgens alter function in parts of the brain connected to emotional processing. If you do lose the ability to cry, it may return in time as your brain becomes more acclimated and you come out of second puberty. Therapy may also help provide you with techniques to cry in a healthy manner.
 Blotchkat
Blotchkat  Willow BIm & Free Palestine William
Willow BIm & Free Palestine William 
Emotional deregulation occurs the most commonly before and immediately after dosing (injections or gel) and results in reduced patience and increased aggression.
Increased Appetite / Eating Capacity
You are going to be hungry. Testosterone cranks the body’s metabolism up significantly, and increased muscle mass means there is more to feed, so you will burn calories faster.
Sleep
Some people report problems with insomnia and having fewer memorable dreams. This is far from universal, however; others feel sleepier and sleep more.
 Elijah ★ (
Elijah ★ (Confidence
Testosterone is known to induce a strong sense of self-confidence in people. Problems seem less significant, self-esteem is stronger, fewer anxieties. Many people report a tendency to be more prone to spark arguments, and more willing to speak out in the face of conflict and self advocate. This does not mean more hostile or argumentative, but simply that one’s tolerance for bullshit is lower.
Extroversion
It’s extremely common for trans people of all types to find themselves much more sociable post-transition. This may simply be a result of no longer having to suppress large portions of their personality, but the aforementioned confidence also plays a role.
Genital Changes
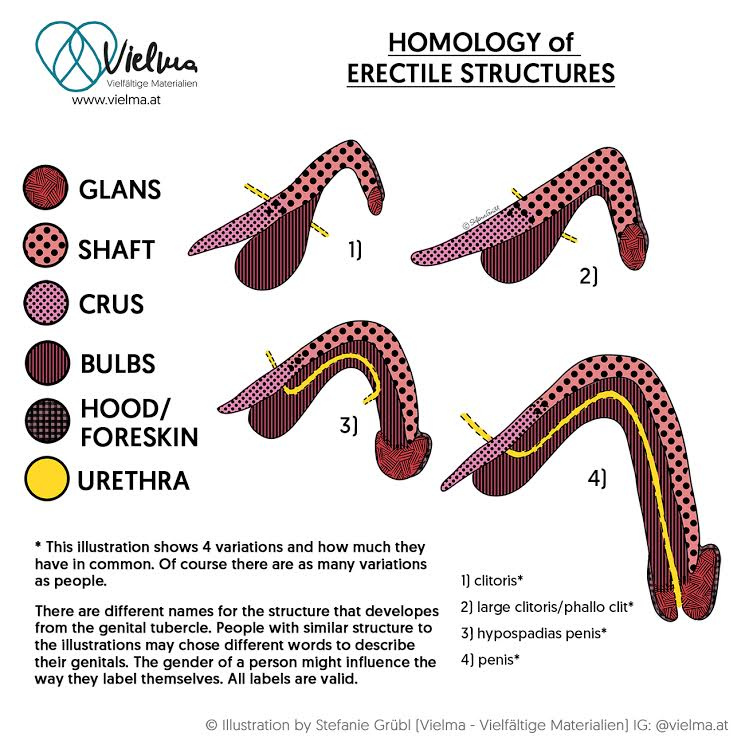
All genitalia are constructed from the same tissues; they are merely organized differently during gestation. Much of the behavior of these tissues is regulated by the hormones one’s body runs on. Skin secretions, textures, sensitivity and erectile behavior are all hormonal expressions. Which means that when you add androgens, these tissues start acting like they are in the shape of a penis and scrotum, even when they aren’t.
Bottom Growth
DHT (mentioned above) plays a critical role in the development of the erectile tissue within the genitals. As DHT levels rise with the increase in testosterone, this will cause the Skene’s gland (sometimes referred to as the female prostate) to swell. This will induce random erections within the clitoris, causing the erectile tissue to grow. The amount of growth varies from person to person, but 1-3 inches is common.
 Aren
Aren  Endeavour @itsendeavour
Endeavour @itsendeavour I’ve been asked what lower/bottom growth is. What actually grows? It’s the bean. The clitoris. Can grow up to 4-5cm. Length/width is purely genetics like it is for cis guys. Looks like a miniature penis. My growth mainly occurred 3 months - 1 year.
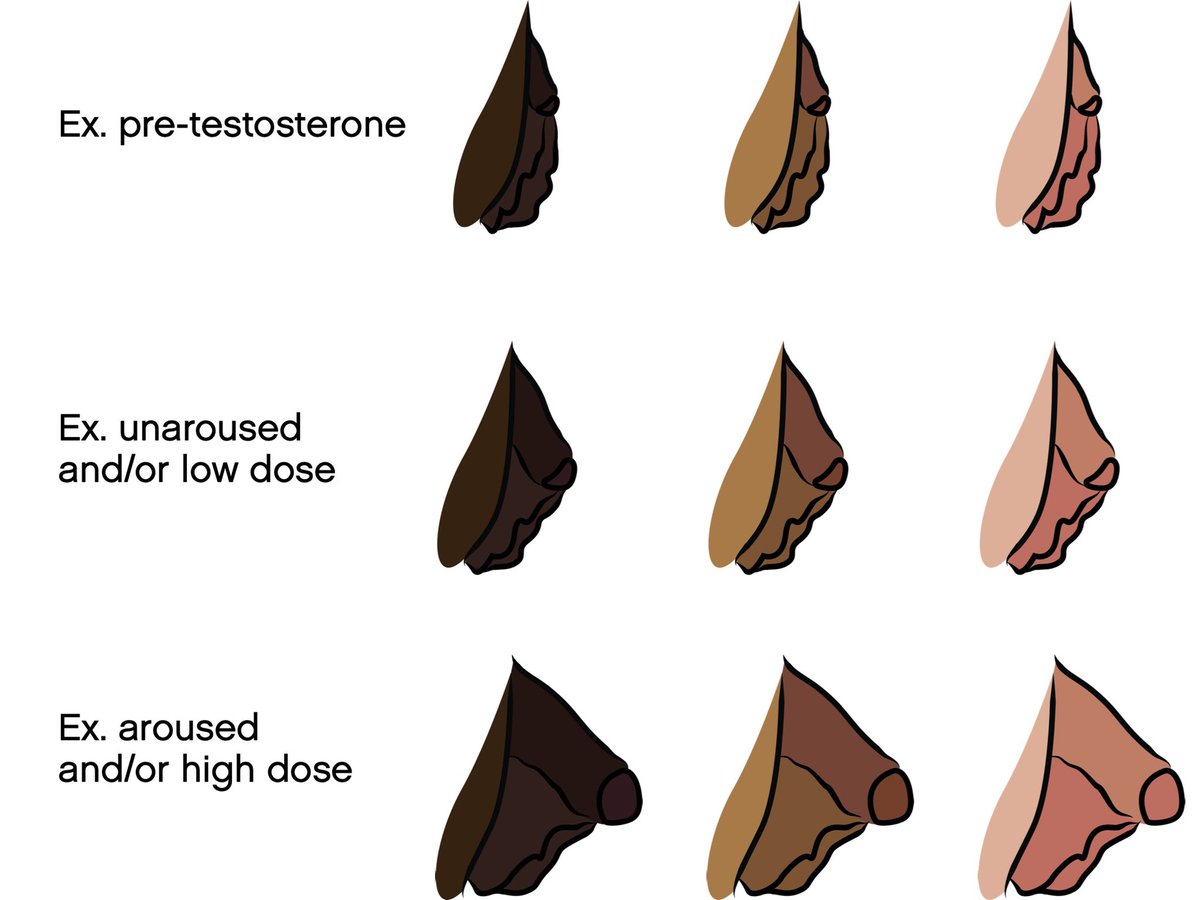 Endeavour @itsendeavour
Endeavour @itsendeavour I grew a foreskin. It got sensitive & painful when having growth spurts, like pins and needles  . Had about 3 growth spurts. Gets erect when aroused and morning erections are a thing. Diagrams from folxhealth.com/library/testos…
. Had about 3 growth spurts. Gets erect when aroused and morning erections are a thing. Diagrams from folxhealth.com/library/testos…
Decreased Lubrication
The clitoral hood and labia will become drier and thicker over time, and the inner labia may also start to grow hair. Self lubrication may reduce substantially, and over time penetration may become painful. Use more lube to avoid tearing and bleeding.
You can also ask your gynecological provider or primary care doctor about vaginal estrogen. The levels of estrogen used in these products are so low, there’s no risk of interference with the effects of testosterone.
Increased Emissions During Climax
With the swelling of the prostate comes more prostate fluid. If you weren’t a squirter before, you may become one now.
Changes in Sensitivity and Response
Erogenous stimulation may become more focused on the head of the clitoris and in stroking of the shaft. Friction in general may become more pleasurable as opposed to vibration. Some people report greater sensitivity during vaginal penetration due to the thinner skin.
Atrophy
Vaginal and uterine atrophy often happens within the first five years, and a hysterectomy may become necessary. Signs of atrophy include a deep throbbing in the lower abdomen and painful cramping without other period symptoms, particularly following intercourse. Vaginal atrophy can be avoided through vaginal estrogen, as well as the use of the same vaginal dilators that AMAB trans people use following vaginoplasty.
Changes to Pap Test
Your internal genitals may develop small amounts of benign prostate tissue, which can range from a couple cells to a “well-developed” gland. The clinical term is androgen-associated prostatic metaplasia. These prostate cells may be misinterpreted as the lesions created by HPV if found on a Pap test, but unlike HPV, the cells in prostatic metaplasia look medically normal and don’t appear to be a cancer risk. If necessary, a biopsy can clearly tell them apart.
Decreased lubrication and atrophy, as discussed above, may also make it physically more difficult to perform the Pap test. The provider may have to exert more force to collect an adequate sample. Your provider can use a smaller speculum to reduce the pain of the procedure. Some providers may allow you to swab your own cervix, but this is not guaranteed.
Increased Sex Drive
Libido will almost certainly go through the roof for the first year or two, with the strongest effects immediately following dosing. You may find yourself more assertive during sex and more prone to being dominant and/or a top.
Orgasm
The “shape” of one’s orgasm can change. Rather than a cascade, it strikes like an explosion from the groin.
Attraction
Testosterone has been shown to increase arousal from visual stimuli. As such, you may notice people of your sexual preference much quicker, especially if you are gynephilic (attracted to the feminine shape).
Cessation of Menstruation
The increase of androgens within the body causes the hypothalamus to down-regulate production of the hormones which control the ovaries. This will reduce total estrogen available, and may halt ovulation. Without ovulation and with lower FSH levels, the uterus will be less inclined to build up and release a lining, causing the cessation of blood flow.
 Moony
Moony You may still experience other period symptoms, however, as the hypothalamus can continue to express other aspects of the monthly cycle. This can even continue following a total hysterectomy, although it is not common.
This does not mean that you are infertile, however. Ovulation can still occur even if you are not menstruating. Additionally, halting testosterone will make the old orbs wake up; they do not die.
Estrogenic Second Puberty 101
What To Expect from Feminizing HRT
This is a compilation of reported medical transition changes collected from testimonials of AMAB trans people taking estrogen-based hormone therapy. This information is gathered from social media and chat rooms. Yes, that means this is all anecdotal, but historically, most of transgender medical study is anecdotal because no one wants to fund transgender medical research.
Note that this is a list of possible changes. There is no guarantee that every person on feminizing HRT will experience all of these. Your age, genetics, medical history, degree of masculinization from natal puberty, and hormone regimen can all have impacts on results. There is also just a degree of randomness — every body is different — and some things can take years to appear.
Breast Growth
Despite public perceptions, the majority of transfems do not pursue breast augmentation, as it often isn’t necessary (and, for many, is not within reach). Every human is born with breast tissue, it simply remains inactive without estrogen to make it grow. Development typically takes 2-5 years, but can continue for more than ten years, just as it does for cisgender women.
Expect aches and pains in the chest, along with lots of tenderness in the area surrounding and behind the areola. Avoid bumping into anything, as it will hurt. Nipples and areolae will become much more sensitive while also becoming larger and darker. You’ll want to invest in some sports bras.
This may be accompanied with lactation. Some secretion is normal and can be expected as milk ducts form and open up, so there is no cause for alarm. However, significant discharge without intentional stimulation may be a sign of a prolactin imbalance, so you should tell your doctor if this happens.
Skin Softening
Testosterone promotes the thickening and toughening of the epidermis, so removing it makes the skin thinner. Additionally, estrogen promotes the production of collagen, which causes skin to become softer and more iridescent. Expect to see more varicose veins on your legs. Tattoos that may have faded over time might become bolder and clearer.
The removal of testosterone also causes a severe drop in skin oils, particularly on the face and scalp. This results in a significant reduction of acne and/or dandruff.
Increased Flexibility
Testosterone causes water retention in ligaments and tendons, rendering them less stretchable. Removing androgens from the body causes the tendons to release those fluids and regain their elasticity.
Slimmer Hands and Wrists
 The author's hands. This change occurred over the course of three and a half years.
The author's hands. This change occurred over the course of three and a half years. As the skin begins to soften and slim down, the hands gradually begin to shrink. Without testosterone, less blood flows to the hands, causing further reduction in tissue sizes. Ring size will drop as fat and fluids move off the fingers. Finger length shortens as ligaments thin and stretch.
Smaller Feet
Much like hands, the feet also experience changes in shape. Androgens encourage more blood flow to the feet, and encourage water build up in cartilage. Estrogens allow the ligaments in the foot to stretch more. Collectively, this causes the arch of the foot to increase, shortening its total length by as much as two centimeters. Many people report a drop of one to two shoe sizes.
Thinner & Softer Fingernails
Fingernails are made of keratin, and many keratin genes are activated by androgen receptors, thus causing thicker fingernails. The loss of testosterone will make the nails thinner and more prone to breakage.
Reduced Body Hair
Do not expect a total cessation of body hair; once the follicles are made terminal by DHT, they remain that way. However, much like fingernails, hair thickness is an expression of keratin genes activated by androgens. Removing testosterone causes the body hairs to become thinner and lighter. Genetics plays a major role in this, however.
Changes in Body Temperature Placement
Androgens encourage extra blood flow to extremities, making them warmer. Because of this, women tend to have warmer core temperatures but lower oral and surface level temperatures. You may see your basal body temperature drop to around 97.6°F (36.4°C).
This, unfortunately, results in a reduced tolerance to cold, so expect to need to layer clothing more frequently, especially since many buildings set their thermostats for male comfort levels.
Changes in Perspiration Patterns
With the above shift in temperature distribution, this also results in a significant change in how one sweats. Sweat becomes more of a full body experience, as opposed to being largely centered on the head and armpits. Underboob sweat becomes a thing.
Reduction and/or Change of Body Odor
A major component in male body odor is the presence of the steroid pheromone androstadienone in sweat. Androstadienone is metabolized directly from testosterone, so halting testosterone removes the source. Without it, sweat takes on a much sweeter smell, which is often attributed to feminine odors.
People taking spironolactone may experience a total cessation of any body odor due to the way the drug alters cortisol uptake within the body.
Reduced Muscle Mass
Androgens stimulate muscle growth, which is why anabolic steroids (which are literally testosterone) are so common amongst bodybuilders. People running on androgens naturally have more muscle mass, particularly in the upper body, without even having to work out. Removing androgens causes that muscle mass to atrophy and makes it harder to gain muscle. This is a major contributor to the feminine shoulder and neck line, as well as the waist line.
With this comes a significant loss in strength. Carrying things becomes more difficult, pickle jars become harder to open.
Fat Redistribution into Feminine Proportions
Androgens encourage the body to deposit fats into the abdomen, while estrogen encourages the body to deposit fats into the thighs, buttocks, and hips. Switching profiles causes new fats to be deposited according to the estrogen profile, and fats that were stored while on androgens break down. This produces the illusion of fat migration as the shape of the body changes. The waistline shrinks and defines itself below the ribs, and the belly becomes softer and flatter.
Because estrogen deposits weight much lower on the body, and the muscle mass in the upper body is lost, this lowers the center of gravity, which alters one’s walking gait. It becomes more natural to cantilever the body with the hips while walking, as opposed to the shoulders.
Facial Feature Changes
Along with body fat migration, fat in the face also migrates. The neck, chin, and jawline thin out while the lips and upper cheeks puff up. The brow and upper eyelids lift, exposing more of the eyeball. Changes in skin and musculature around the eye can alter the shape of the eyeball, changing focal depth and altering vision clarity. The color of the eyes may also change and become bolder, as testosterone causes the pigmentation in the iris to fade.
This is an extremely subtle and slow moving process that takes years, and it is easy to think nothing is changing at all. Take selfies to compare.
Changes to Scalp Hair
With the removal of androgens, blood flow to the scalp increases. Follicles that had been lost to male pattern baldness may reactivate, causing some return of the hairline and a filling-in of bald spots. Scalp hair becomes thicker and follicles grow stronger, allowing hair to grow to longer lengths.
With this thickening, curliness may become more pronounced, and a change in hair color may also occur. You might find your hair taking on a texture more like your mother’s than your father’s.
Anterior Pelvic Tilt
As musculature atrophies, ligament flexibility increases, and weight shifts lower on the body, the orientation of the pelvic bone in relation to the spine and femurs rotates forward — not by much (only about 10-20 degrees), but enough to cause a change in the alignment of the spine and hips, increasing the arch of the back and causing the buttocks to jut out more. The added arch to the back can cause a relative drop in total height, between 1 and 2 inches (2-5 cm) depending on pelvic shape.
Note: this is NOT the same as the hip rotation that occurs in AFAB puberty and during pregnancy. That is the result of migration of bone cells, altering the shape of the pelvic bone itself. However, hip rotation can occur if the person is young enough to still be within initial puberty, where the body is producing elevated human growth hormone. There have also been examples of hip rotation happening over long periods of time in trans elders. In 2017 an 80 year old trans woman reported on reddit that over the course of her 30 years on HRT, her doctor observed changes in her pelvis consistent with female hip rotation.
Reduced Tolerance of Caffeine, Alcohol, and/or Psychotropics
Less body mass means less blood to dilute chemicals into. Losing testosterone also means a slower metabolic rate, decreasing the speed at which toxins are reduced from the bloodstream. Some anti-androgens also put strain on the liver, further reducing how quickly chemicals are processed.
Mental Changes
As covered in the Biochemical Dysphoria section, brains can be wired for a certain hormone profile, and running on the wrong profile is like using a laptop with low batteries or an overheated processor. Starting HRT almost universally results in a cessation of depersonalization and derealization (DPDR) symptoms within the first two weeks. A mental fog lifts, and it becomes easier to concentrate on complex concepts (assuming you don’t also have other mental processing difficulties such as ADHD).
ADHD
If you have ADHD, there may be some changes in your symptoms. Androgens amplify dopamine receptor function, so reducing testosterone can reduce the activation potential for dopamine in the brain. Dopamine is a key neurotransmitter in the behavior of working memory, the short-term memory of the brain. Less working memory means you become more prone to distractions and have more difficulty maintaining cognitive load.
The good news is that estradiol prompts the brain to produce MORE dopamine.
Authors Note:
There is a known problem with spironolactone hampering working memory due to its effects on mineralocorticoids. This can significantly worsen ADHD issues and make it much harder to maintain focus or be aware of your surroundings. I was involved in a car accident in 2017 that I blame on spiro fog.
Emotional Expansion
The alleviation of DPDR almost universally is accompanied with a much broader capacity for emotion and expression. The stoicism and dissociation lifts and emotions land with much greater intensity. Highs are higher and lows are lower. Those who may have been unable to cry before transition gain it back, both for sadness and for joy.
Unfortunately, this also means that, if you had trauma from events earlier in life (and who doesn’t), you may start to experience PTSD episodes. This is why it is good (and, in some places, required) to have a therapist.
Mood Swings
As estrogen levels fluctuate between doses, you may experience noticeable and sometimes dramatic shifts in your mood. Unexplained crying happens; PMS rage happens; be ready for it.
Appetite
Many people report being unable to eat as much as they could pre-transition. The loss of lean muscle in the arms and shoulders means that the body has a reduced capacity for burning lipids, and as such the fullness sensation occurs earlier.
However, progesterone increases mitochondrial function within the body, boosting metabolic rate. This can cause an increase in appetite as the body attempts to replenish calories burned.
That said, you may find yourself unable to eat as much food as you could before. Many report that they become full/satisfied sooner than before.
Sleep
Many people report having better sleep patterns after starting HRT. This is likely a factor of the alleviation of DPDR, as it seems to occur in both AMAB and AFAB trans people. That said, initiating progesterone can significantly improve sleep, allowing for deeper sleep and more dreaming.
Extroversion
It’s extremely common for trans people of all types to find themselves much more sociable post-transition. This may not actually be a factor of hormone therapy, however, and may simply be a result of no longer having to suppress large portions of their personality.
Sensory Enhancements
Transgender HRT has been shown several times to cause changes in the distribution of gray matter and white matter within the brain for trans people on both forms of HRT. New structures and neuro-pathways are formed as a result of the shift in hormone profiles, and this results in changes of sensory perception. These are some of the changes that have been observed and reported, but it is not clear if this is a function of the hormones themselves, or a factor of the brain receiving the hormones it is wired for.
- Improved sense of smell, especially of other bodies. Human sweat becomes very discernible — even overpowering at times.
- Improved color perception. Colors may become bolder, richer.
- Improved spatial awareness. Many trans people experience poor proprioception and a tendency towards clumsiness that goes away after starting HRT.
- Changes in perception of taste. Certain foods become more or less palatable; cilantro, for example, may become more or less soapy. Increased tolerance of capsaicin (spicy peppers). Chocolate and wine become more flavorful.
Users of spironolactone often develop strong cravings for foods high in salt, such as pickles, olives, or potato products. This is because spiro is a potassium-sparing diuretic which causes you to pee out all your sodium. The brain creates cravings to encourage you to replace that sodium.
Spatial Shift, Reduced Confidence
There is a very frequently reported experience of feeling smaller within the world, even when wearing heels. People taller than you seem to tower over you, and spaces feel larger.
People have also reported a tendency to be less prone to start arguments, as well as a desire to avoid confrontation rather than create it. Testosterone has been shown to increase a person’s sense of confidence, and removing it has the opposite effect.
Genital Changes
All genitalia are constructed from the same tissues; they are merely organized differently during gestation. Much of the behavior of these tissues is regulated by the hormones one’s body runs on. Skin secretions, textures, sensitivity and erectile behavior are all hormonal expressions, which means that when you remove androgens and add estrogens, these tissues start acting like they are in the shape of a vulva, even though they aren’t.
Increased Sensitivity
The skin on the glans and shaft becomes much thinner and fragile, more prone to tearing and irritation, while also becoming significantly more sensitive to touch. The entire organ also becomes much more sensitive to pressure, and vibration becomes a better form of stimulation over stroking, which may become painful.
Moisture and Feminine Odor
The skin along the shaft begins to secrete the same fluids as the vaginal canal, particularly during arousal (yes, trans girls get wet). These fluids encourage the development of the same microbiome that develops within the vaginal canal. The combination of these factors means that odor (and taste) of the penis changes to align more to that of a vulva.
Color and Texture Changes
The scrotum is an analog of the outer and inner labia, and takes on a softer, more velvety texture, extending down into the perineum. The skin along the perineal raphe (the vertical line where the vulva opening had been before the scrotum formed) will also darken. Some people experience a kind of striping pattern along the scrotum.
Fewer Erections
Without free-floating testosterone, the levels of DHT in the bloodstream drop significantly. DHT plays a major role in the stimulation of random erections during sleep through the enlargement of the prostate, and these erections are what is responsible for the maintenance of the erectile tissue. Without DHT, the prostate shrinks again, and random erections cease (no more morning wood).
However, this means that the erectile tissue will begin to atrophy. Prolonged atrophy will result in shrinkage of the entire organ, for better or worse. The shape of the penis changes as this occurs, often becoming more conical. The glans is the first part to shrink and may lose the ability to become rigid. Penetrative sex may become more difficult, and erections themselves may become painful.
This can be countered by regularly inducing erections, but that may become more and more difficult as time goes on.
Clear Ejaculate
The majority of the liquid that makes up ejaculate originates in the prostate. It is a completely clear fluid, with a slimy texture. The white color and stickiness that is usually attributed to male ejaculate is caused by semen and seminal fluid from the testicles. The production of both semen and seminal fluid is a product of testicle function, so as the testicles shut down (either because of anti-androgens or from estrogen dominance), these fluids halt, leaving only the prostate fluid.
Some people lose even that, and stop having any emissions at all during orgasm.
Needless to say, this comes with sterility. Contrary to what some sources report, this is NOT permanent, and many people have been able to restore testicle functionality by halting hormone therapy, either for detransition or for reproductive purposes.
Testicle Atrophy
Once the testes have stopped functioning, the cells start to atrophy, shrinking over time. This atrophy may be accompanied with pain, sometimes in the form of a soreness or a dull throbbing sensation, or sometimes as registering as little sparks of pain that travel along the perineal nerve from the testicles down to the rectum.
Sexual Changes
Initial start of HRT may result in a total loss of sex drive as testosterone levels plummet. This can last 3-12 months, and, in some cases, doesn’t return at all. Starting progesterone often serves as a catalyst for its return. If/when sex drive comes back, the new libido may be a completely different experience that one may not recognize at first.
Heightened Erogenous Zones
Human Erogenous Zones:
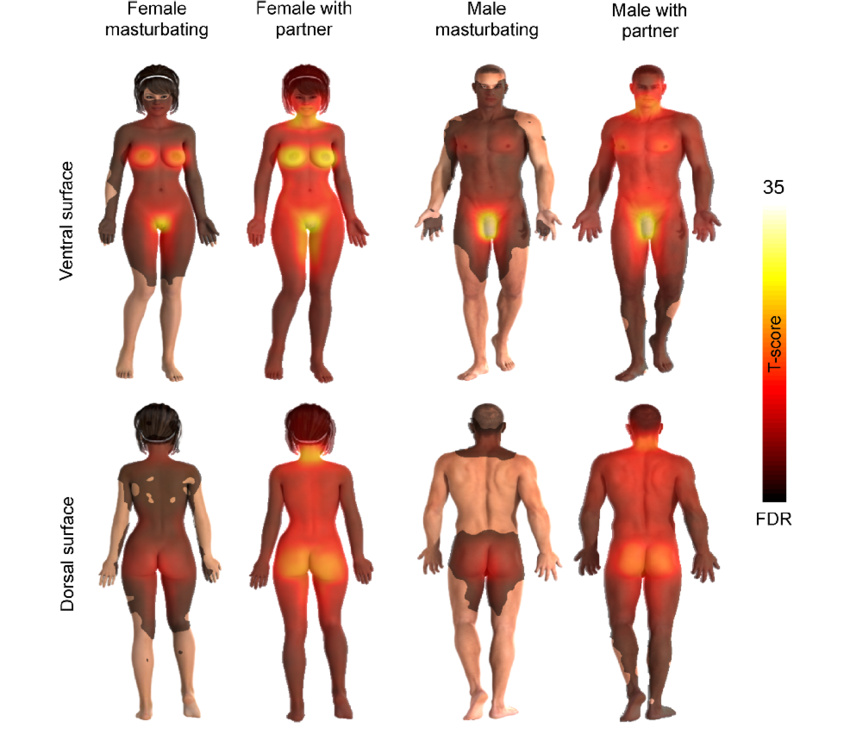
The entire body becomes more responsive to touch, and with that unlocks stronger erogenous zones. Breasts, abdomen, inner thighs, and neck, in particular, become more arousal-inducing.
Orgasm
Orgasm changes significantly, both in the way it builds and how it is experienced (see link above), but additionally, if one is lucky, they will gain the ability to become multi-orgasmic with no refractory period. The cost of this is that orgasm may become harder to achieve, and one has to re-learn how to reach it. It also becomes easier to reach with a partner, which may have been the opposite before.
Attraction
It is not at all unheard of for a transgender person to experience a change in their sexual orientation with transition. This is almost always the result of the removal of self-imposed mental barriers, but hormone therapy often plays a role in that removal. In most cases this simply involves an expansion of ones attraction, from monosexual to bi/pansexual, but some people also discover that their attraction was largely rooted in self-interest and that their true attraction is reversed.
Cyclical Period-like Symptoms
Obviously, we do not mean blood flow; that would be ludicrous. Symptoms vary greatly (just as they do in cisgender women) and typically last for 2-4 days, repeating every 26-32 days (though some report experiencing it every two weeks). This happens independent of medication dosing schedules. The use of a period tracker app like Clue can reveal the pattern.
- Cramping in the intestine and abdominal muscles, ranging from a slight flutter in the gut to strong painful spasms.
- Bloating and water retention
- Gas, diarrhea and other intestinal issues.
- Emotional instability, mood swings and irrational thoughts
- Heightened depression and dysmorphia
- Depersonalization or dissociation.
- Increased dysphoria
- Irritability (PMS)
- Muscle and joint aches and pains
- Breast engorgement and nipple tenderness
- Acne
- Fatigue
- Appetite changes and spontaneous cravings (see: chocolate cravings)
- Spontaneous shifts in libido
- Changes in genital odor
No, there have not yet been studies on this yet, but it is reported by far, far too many individuals to be an anomaly (including by yours truly), and has been confirmed by multiple people’s own doctors. There is also precedent of this happening with cisgender women who have had hysterectomies (I personally know two cisgender women who have cycles but do not menstruate, without any medical intervention).
Running on estrogen and progesterone activates a gene sequence which instructs the hypothalamus to attempt to cycle ovary and uterine behavior just as it does in female-assigned individuals, regardless of the absence of ovaries or a uterus. This cycle affects numerous organs and subsystems in the body, causing the release of a variety of different hormones and enzymes that can affect function and even behavior.
A more thorough explanation of this will be coming in a later update to the site.
Choice
What is choice? No, I’m not talking about free will and fate. That is not a subject within the scope of this essay. However, in the context of gender, I do believe it is important to consider the processes that drive us to make decisions.
In the philosophy of decision theory, choice is broken down into two pieces: preferences and prospects. Prospects are the different paths that lay before us — the unresolved potential of any given choice. Preferences are our internal factors that drive us towards one prospect over another. Sometimes these are overtly clear, rational choices that we can describe easily with language. These motivations come from what is coined as the rational mind. Just as often, however, these preferences come to us without clear reasoning, stemming from our past experiences, our biochemical driving forces, or instinctual drives that exist below all of that. Sometimes our preference is just a gut feeling, deep inside. Proponents of mindfulness refer to this as the emotional mind.
Regardless of where a preference originates from, however, it is shaped by its position between two poles. Pleasure and discomfort. Peace and dissonance. Euphoria and dysphoria. Everything we do, every choice we make, comes from either positive or negative responses. When faced with two options, we will select the one we find most beneficial or least harmful to our own internal needs.
What does this have to do with gender? A person’s gender is not a choice; it comes from somewhere deep inside them at a level of the brain’s function that is not subject to change. There are factors which may result in fluctuation of a person’s perception of their gender (as in genderfluid individuals and those with dissociative identities), and a person may change how they describe their gender over time, but no one chooses their gender identity. We only choose how to present it to the rest of the world.
Those choices, those preferences, are driven by what feels good and what feels bad. A person who chooses to publicly identify as a gender different from the one assigned to them at their birth is making that choice based on what feels right to do. A person defending that identity does so based on what feels wrong. We make these choices against the social stigma and discrimination that comes with the transgender label, and indeed a not-insignificant number of trans people may choose to go stealth and abandon that label once it is safe to do so. Even among those who are not stealth, many trans people accept the safety of being presumed cisgender, and take no effort to break people of that presumption. That is, again, a choice. Being visibly trans produces a negative experience for them.
There are those who find the notion that euphoria and dysphoria are central motivators behind gender variance to be uncomfortable; one could even say they experience dysphoria at the concept of dysphoria. To them, ask, if you believe you do not have dysphoria, why did you take on the mantle of the trans label? That choice did not happen in a vacuum; even if your motivations stem entirely from happy feelings, ask yourself how you feel when your gender is not respected. How do you feel when others invalidate your identity?
Is it not a state of unease or generalized dissatisfaction?
That’s dysphoria, baby.
We’re here, we’re queer.
Every single year, we get new studies that show an increase in the size of the transgender population. As awareness continues to grow, more and more people are realizing what has been wrong with their lives and are coming out of the closet. People who transitioned decades ago are coming out of stealth. GLAAD estimates as much as 3% of the population could be transgender, and I have seen numbers as high as 5% or even 10% from more liberal estimations. The more we come to understand about gender, the more language we gain to describe gender, the more people realize that the rigid Male and Female sexual structure that we have been forced into is false.
Yet all this change frightens people. It frightens conservatives who see their patriarchal social structures dissolving under the new understanding of gender. It frightens old-school transgender people who transitioned under the Harry Benjamin rules and now see so many people easily obtaining what they had to act and lie and manipulate to achieve. They fear that if anyone can be trans, the public will stop taking trans people seriously. It frightens the misogynistic or misandristic trans-exclusionary groups that fight so hard to invalidate transgender rights because they think, if anyone can be a man or a woman, their status as a man or a woman is harmed.
There is no such thing as a “Transtrender”.
There is no such thing as “Rapid Onset Gender Dysphoria”.
There is no such thing as people “transing” kids.
These mentalities have to stop.